

Addressing the contribution of previously described genetic and epidemiological risk factors associated with increased prostate cancer risk and aggressive disease within men from South Africa
- PMID: 24373635
- PMCID: PMC3882498
- DOI: 10.1186/1471-2490-13-74
Addressing the contribution of previously described genetic and epidemiological risk factors associated with increased prostate cancer risk and aggressive disease within men from South Africa
Abstract
Background: Although African ancestry represents a significant risk factor for prostate cancer, few studies have investigated the significance of prostate cancer and relevance of previously defined genetic and epidemiological prostate cancer risk factors within Africa. We recently established the Southern African Prostate Cancer Study (SAPCS), a resource for epidemiological and genetic analysis of prostate cancer risk and outcomes in Black men from South Africa. Biased towards highly aggressive prostate cancer disease, this is the first reported data analysis.
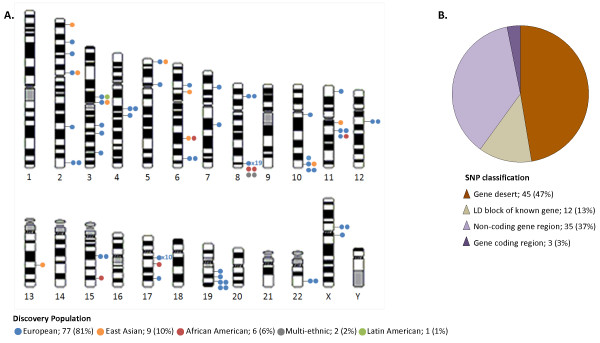
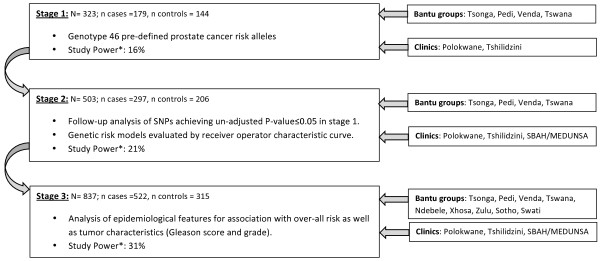
Methods: The SAPCS is an ongoing population-based study of Black men with or without prostate cancer. Pilot analysis was performed for the first 837 participants, 522 cases and 315 controls. We investigate 46 pre-defined prostate cancer risk alleles and up to 24 epidemiological measures including demographic, lifestyle and environmental factors, for power to predict disease status and to drive on-going SAPCS recruitment, sampling procedures and research direction.
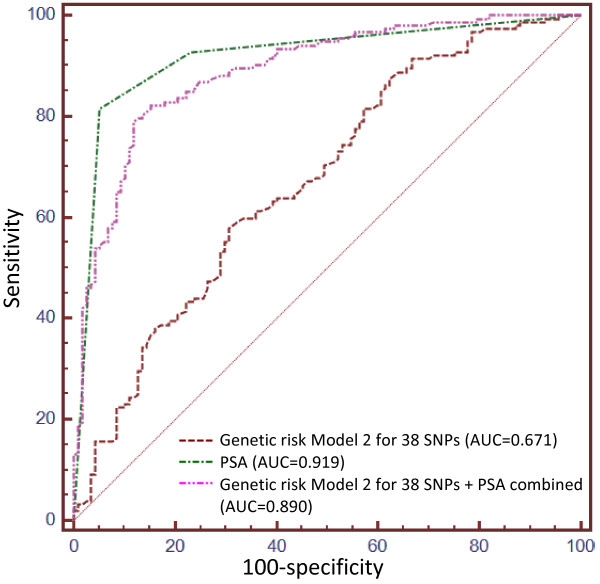
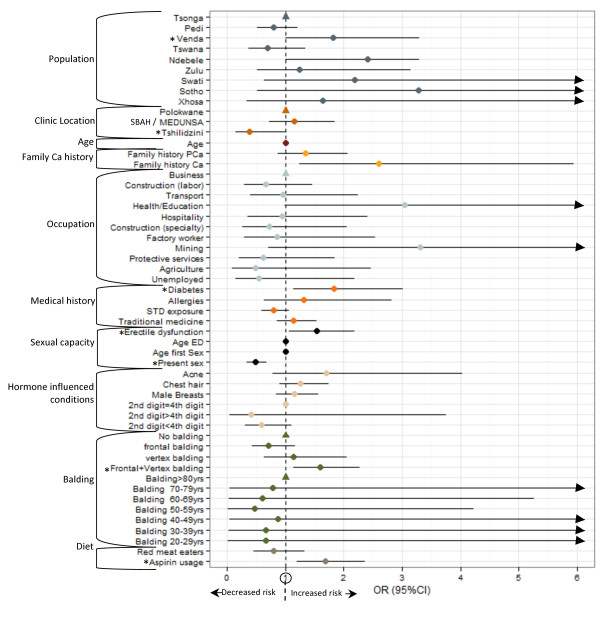
Results: Preliminary results suggest that no previously defined risk alleles significantly predict prostate cancer occurrence within the SAPCS. Furthermore, genetic risk profiles did not enhance the predictive power of prostate specific antigen (PSA) testing. Our study supports several lifestyle/environmental factors contributing to prostate cancer risk including a family history of cancer, diabetes, current sexual activity and erectile dysfunction, balding pattern, frequent aspirin usage and high PSA levels.
Conclusions: Despite a clear increased prostate cancer risk associated with an African ancestry, experimental data is lacking within Africa. This pilot study is therefore a significant contribution to the field. While genetic risk factors (largely European-defined) show no evidence for disease prediction in the SAPCS, several epidemiological factors were associated with prostate cancer status. We call for improved study power by building on the SAPCS resource, further validation of associated factors in independent African-based resources, and genome-wide approaches to define African-specific risk alleles.
Figures
References
-
- Wever EM, Draisma G, Heijnsdijk EA, Roobol MJ, Boer R, Otto SJ, de Koning HJ. Prostate-specific antigen screening in the United States vs in the European randomized study of screening for prostate cancer-Rotterdam. J Natl Cancer Inst. 2010;13(5):352–355. doi: 10.1093/jnci/djp533. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
