

Progesterone in experimental permanent stroke: a dose-response and therapeutic time-window study
- PMID: 24374329
- PMCID: PMC3914469
- DOI: 10.1093/brain/awt319
Progesterone in experimental permanent stroke: a dose-response and therapeutic time-window study
Abstract
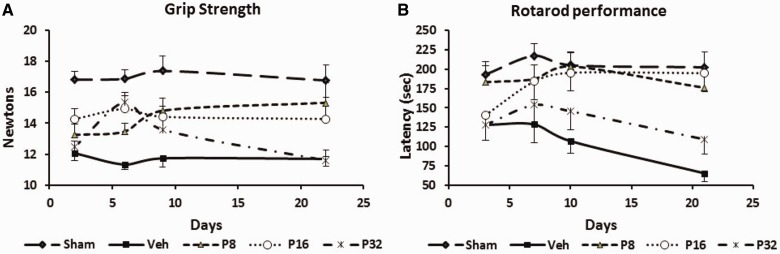
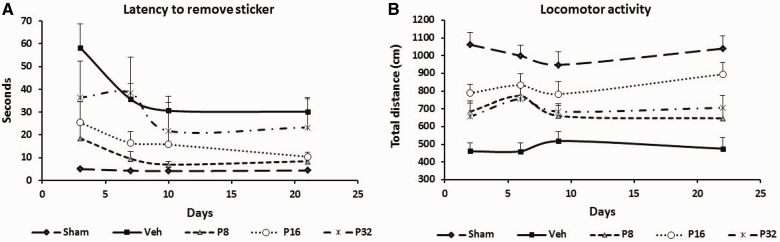
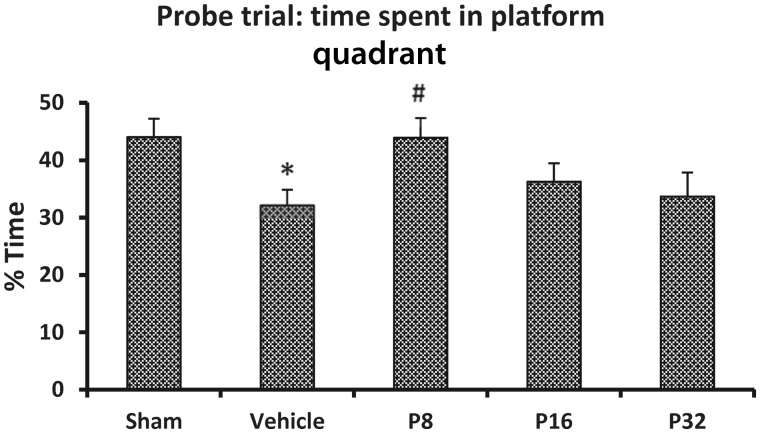
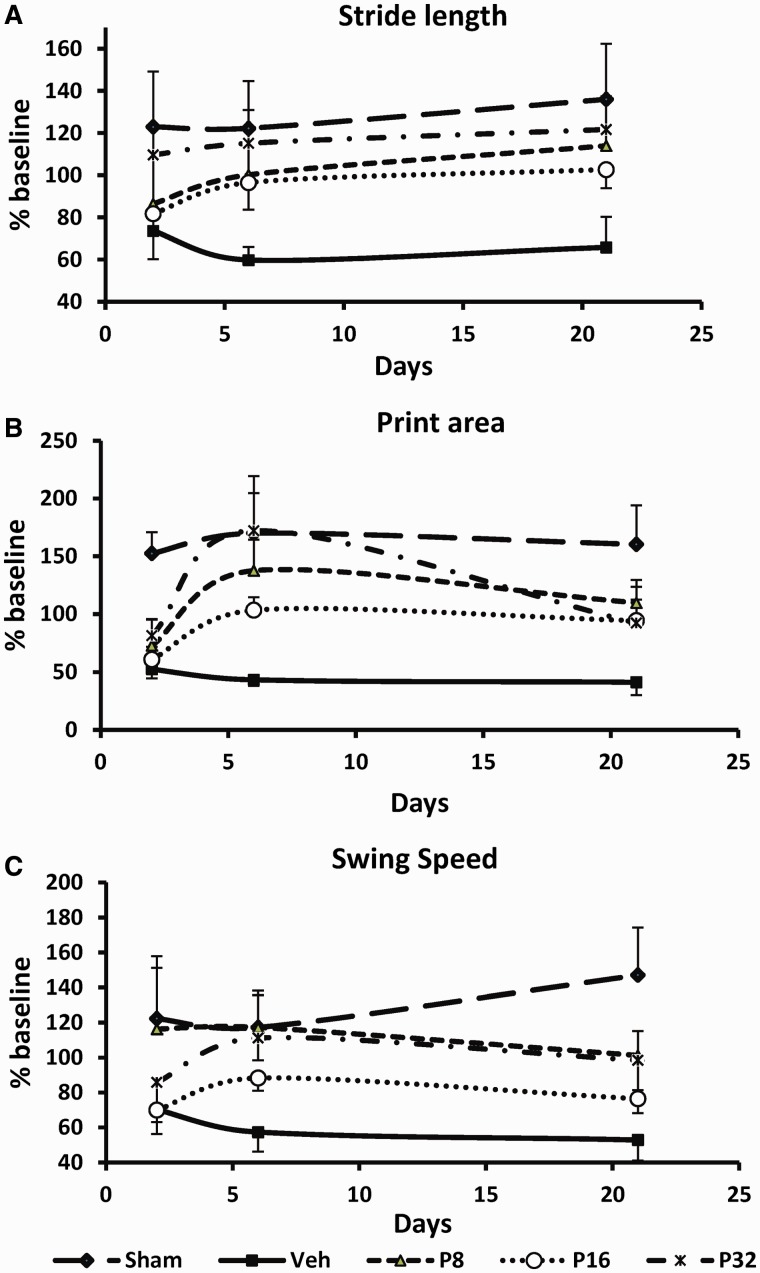
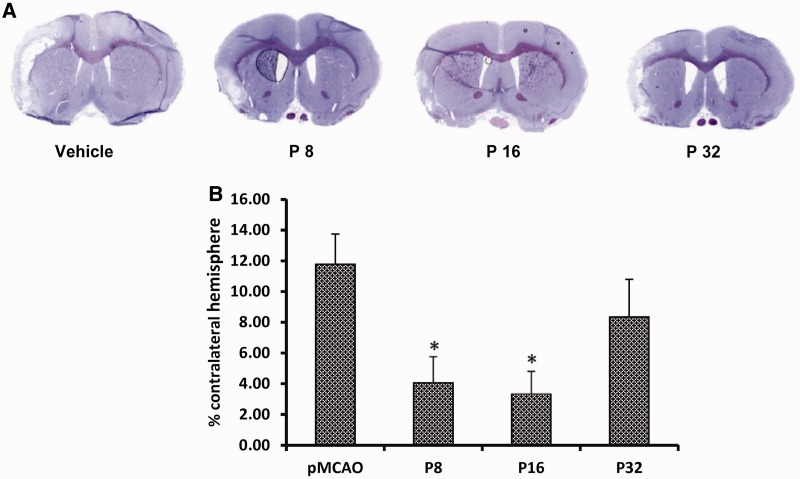
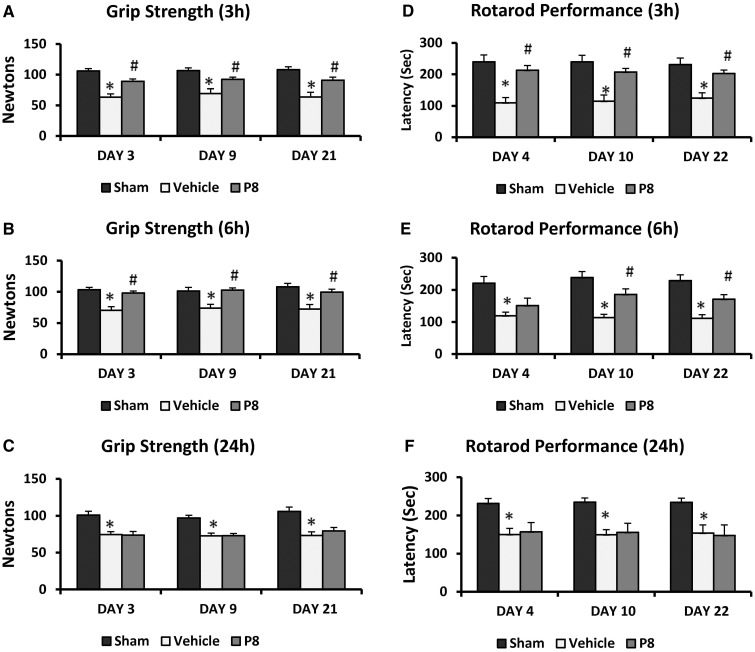
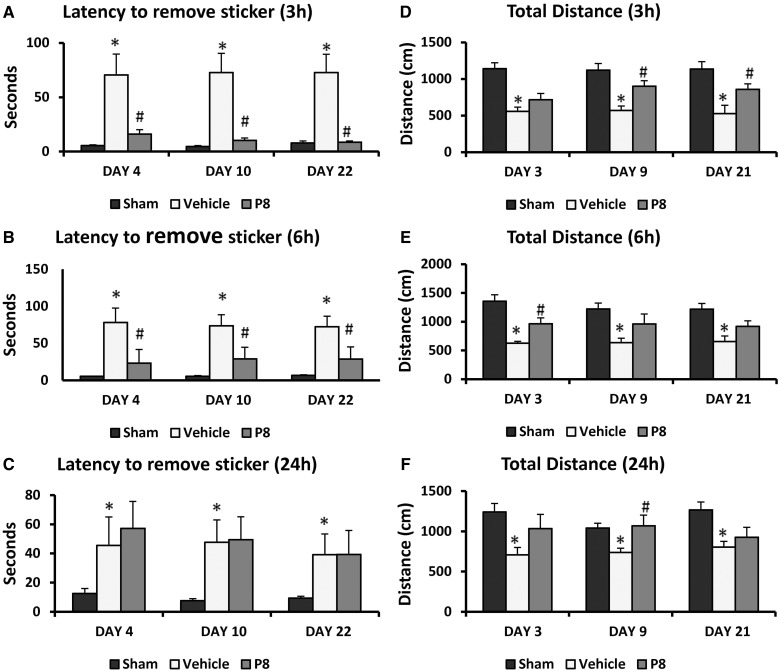
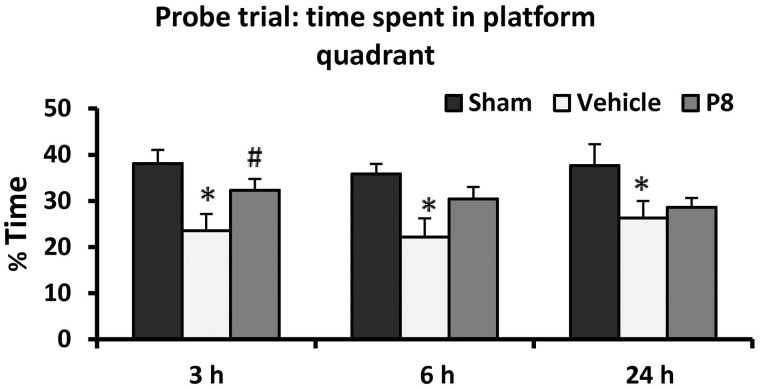
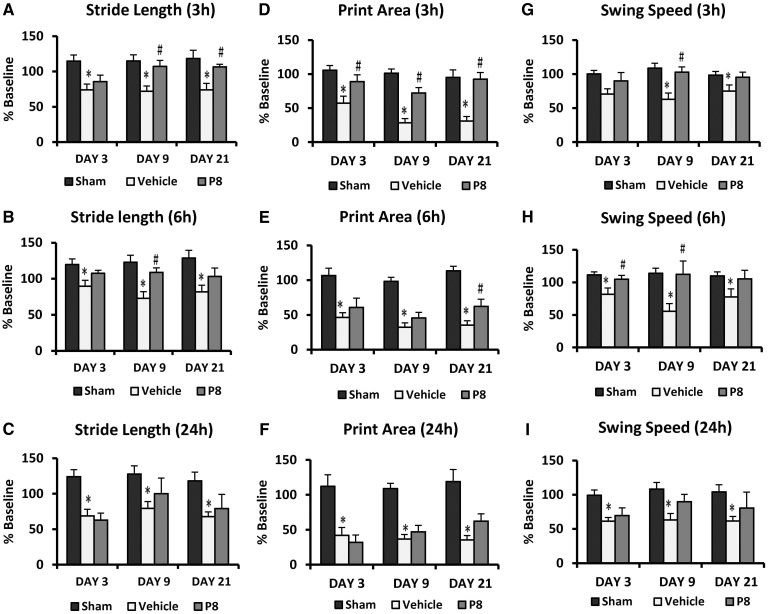
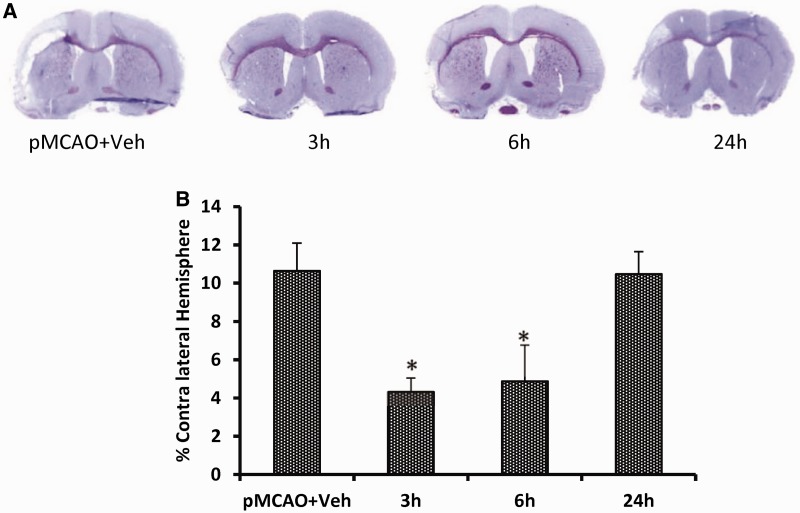
Currently, the only approved treatment for ischaemic stroke is tissue plasminogen activator, a clot-buster. This treatment can have dangerous consequences if not given within the first 4 h after stroke. Our group and others have shown progesterone to be beneficial in preclinical studies of stroke, but a progesterone dose-response and time-window study is lacking. We tested male Sprague-Dawley rats (12 months old) with permanent middle cerebral artery occlusion or sham operations on multiple measures of sensory, motor and cognitive performance. For the dose-response study, animals received intraperitoneal injections of progesterone (8, 16 or 32 mg/kg) at 1 h post-occlusion, and subcutaneous injections at 6 h and then once every 24 h for 7 days. For the time-window study, the optimal dose of progesterone was given starting at 3, 6 or 24 h post-stroke. Behavioural recovery was evaluated at repeated intervals. Rats were killed at 22 days post-stroke and brains extracted for evaluation of infarct volume. Both 8 and 16 mg/kg doses of progesterone produced attenuation of infarct volume compared with the placebo, and improved functional outcomes up to 3 weeks after stroke on locomotor activity, grip strength, sensory neglect, gait impairment, motor coordination and spatial navigation tests. In the time-window study, the progesterone group exhibited substantial neuroprotection as late as 6 h after stroke onset. Compared with placebo, progesterone showed a significant reduction in infarct size with 3- and 6-h delays. Moderate doses (8 and 16 mg/kg) of progesterone reduced infarct size and improved functional deficits in our clinically relevant model of stroke. The 8 mg/kg dose was optimal in improving motor, sensory and memory function, and this effect was observed over a large therapeutic time window. Progesterone shows promise as a potential therapeutic agent and should be examined for safety and efficacy in a clinical trial for ischaemic stroke.
Keywords: dose response; functional recovery; progesterone; stroke; therapeutic time window.
Figures
Comment in
-
A (mini) pill for stroke?Brain. 2014 Feb;137(Pt 2):311-2. doi: 10.1093/brain/awt365. Brain. 2014. PMID: 24501074 No abstract available.
References
-
- Alkayed NJ, Murphy SJ, Traystman RJ, Hurn PD, Miller VM. Neuroprotective effects of female gonadal steroids in reproductively senescent female rats. Stroke. 2000;31:161–8. - PubMed
-
- Asbury ET, Fritts ME, Horton JE, Isaac WL. Progesterone facilitates the acquisition of avoidance learning and protects against subcortical neuronal death following prefrontal cortex ablation in the rat. Behav Brain Res. 1998;97:99–106. - PubMed
-
- Betz AL, Coester HC. Effect of steroids on edema and sodium uptake of the brain during focal ischemia in rats. Stroke. 1990;21:1199–204. - PubMed
-
- Bitran D, Dowd JA. Ovarian steroids modify the behavioral and neurochemical responses of the central benzodiazepine receptor. Psychopharmacology (Berl) 1996;125:65–73. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
