

Sensitivity of Medicare Claims to Identify Cancer Recurrence in Elderly Colorectal and Breast Cancer Patients
- PMID: 24374419
- PMCID: PMC4072852
- DOI: 10.1097/MLR.0000000000000058
Sensitivity of Medicare Claims to Identify Cancer Recurrence in Elderly Colorectal and Breast Cancer Patients
Abstract
Background: Researchers are increasingly interested in using observational data to evaluate cancer outcomes following treatment, including cancer recurrence and disease-free survival. Because population-based cancer registries do not collect recurrence data, recurrence is often imputed from health claims, primarily by identifying later cancer treatments after initial treatment. The validity of this approach has not been established.
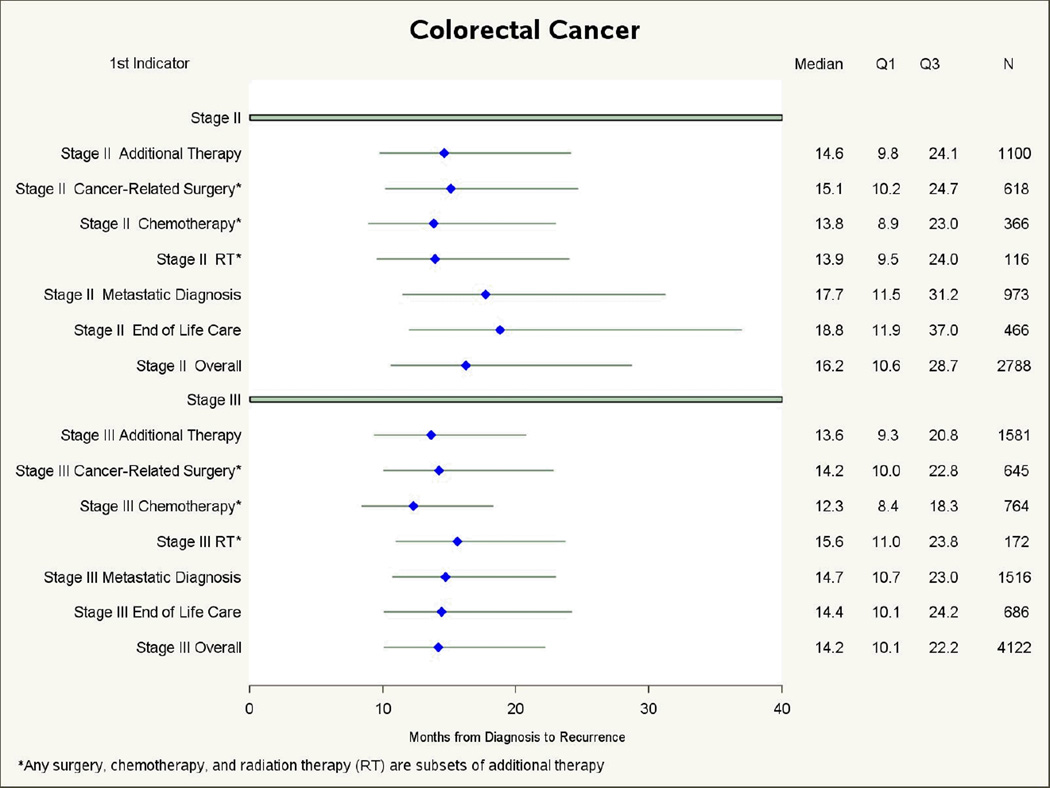
Research design: We used the linked Surveillance, Epidemiology, and End Results-Medicare data to assess the sensitivity of Medicare claims for cancer recurrence in patients very likely to have had a recurrence. We selected newly diagnosed stage II/III colorectal (n=6910) and female breast cancer (n=3826) patients during 1994-2003 who received initial cancer surgery, had a treatment break, and then died from cancer in 1994-2008. We reviewed all claims from the treatment break until death for indicators of recurrence. We focused on additional cancer treatment (surgery, chemotherapy, radiation therapy) as the primary indicator, and used multivariate logistic regression analysis to evaluate patient factors associated with additional treatment. We also assessed metastasis diagnoses and end-of-life care as recurrence indicators.
Results: Additional treatment was the first indicator of recurrence for 38.8% of colorectal patients and 35.2% of breast cancer patients. Patients aged 70 and older were less likely to have additional treatment (P < 0.05), in adjusted analyses. Over 20% of patients either had no recurrence indicator before death or had end-of-life care as their first indicator.
Conclusions: Identifying recurrence through additional cancer treatment in Medicare claims will miss a large percentage of patients with recurrences; particularly those who are older.
Figures




References
-
- Earle CC, Nattinger AB, Potosky AL, Lang K, Mallick R, Berger M, Warren JL. Identifying cancer relapse using SEER-Medicare data. Med Care. 2002 Aug;40(8 Suppl):IV-75–IV-81. PubMed PMID: 12187172. - PubMed
-
- Lamont EB, Herndon JE, 2nd, Weeks JC, Henderson IC, Earle CC, Schilsky RL, Christakis NA Cancer and Leukemia Group B. Measuring disease-free survival and cancer relapse using Medicare claims from CALGB breast cancer trial participants (companion to 9344) J Natl Cancer Inst. 2006 Sep 20;98(18):1335–1338. Erratum in: J Natl Cancer Inst. 2006 Nov 1;98(21):1584. J Natl Cancer Inst. 2008 Jan 2;100(1):70. PubMed PMID: 16985253. - PMC - PubMed
-
- Chen AB, D'Amico AV, Neville BA, Steyerberg EW, Earle CC. Provider case volume and outcomes following prostate brachytherapy. J Urol. 2009 Jan;181(1):113–118. discussion 118. Epub 2008 Nov 13. PubMed PMID: 19012905. - PubMed
-
- Cheng L, Swartz MD, Zhao H, Kapadia AS, Lai D, Rowan PJ, Buchholz TA, Giordano SH. Hazard of recurrence among women after primary breast cancer treatment--a 10-year follow-up using data from SEER-Medicare. Cancer Epidemiol Biomarkers Prev. 2012 May;21(5):800–809. Epub 2012 Mar 16. Erratum in: Cancer Epidemiol Biomarkers Prev. 2012 Sep;21(9):1604-5. PubMed PMID: 22426147. - PubMed
-
- Cohen JH, Schoenbach VJ, Kaufman JS, Talcott JA, Schenck AP, Peacock S, Symons M, Amamoo MA, Carpenter WR, Godley PA. Racial differences in clinical progression among Medicare recipients after treatment for localized prostate cancer (United States) Cancer Causes Control. 2006 Aug;17(6):803–811. PubMed PMID: 16783608. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
