

Diabetes and weight in comparative studies of bariatric surgery vs conventional medical therapy: a systematic review and meta-analysis
- PMID: 24374842
- PMCID: PMC3916703
- DOI: 10.1007/s11695-013-1160-3
Diabetes and weight in comparative studies of bariatric surgery vs conventional medical therapy: a systematic review and meta-analysis
Abstract
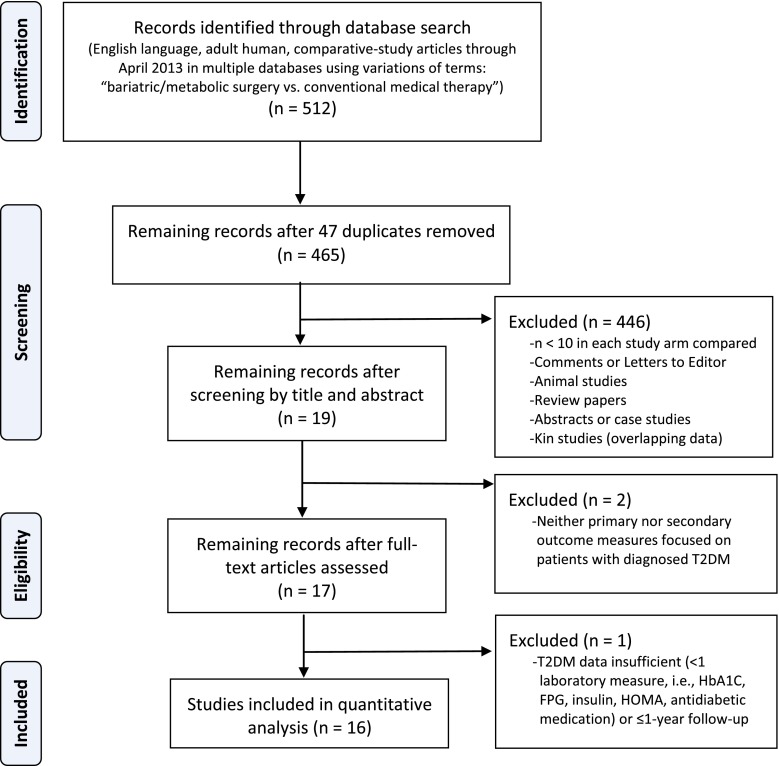
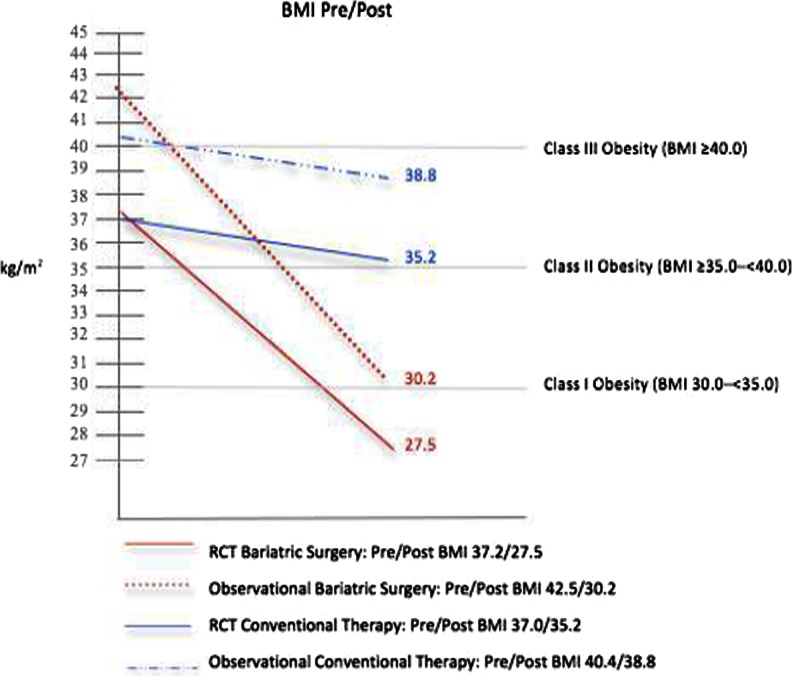
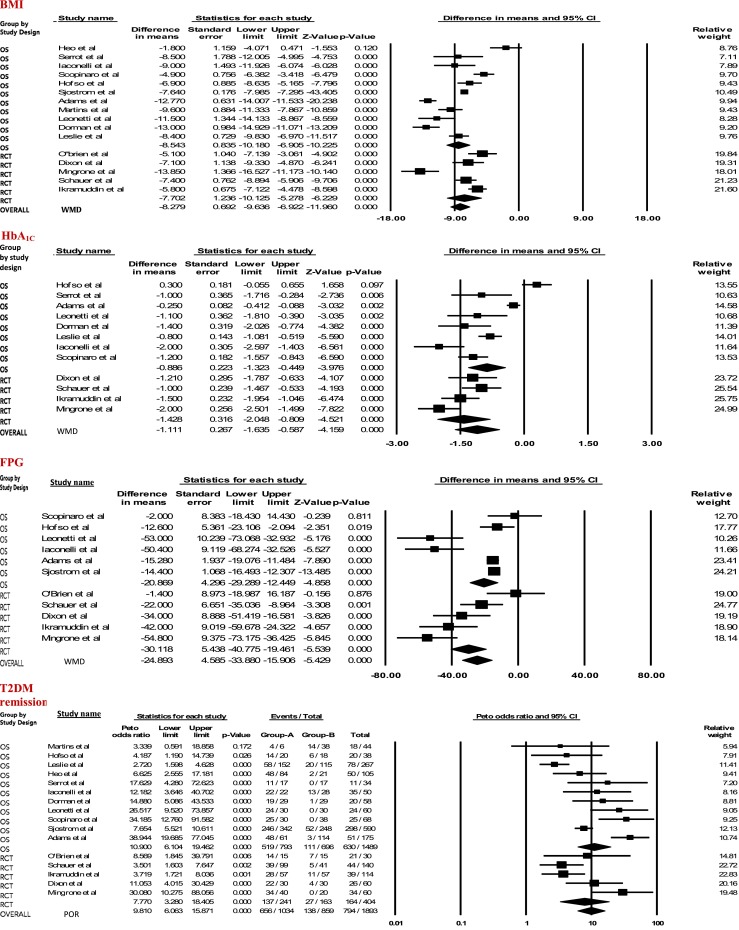
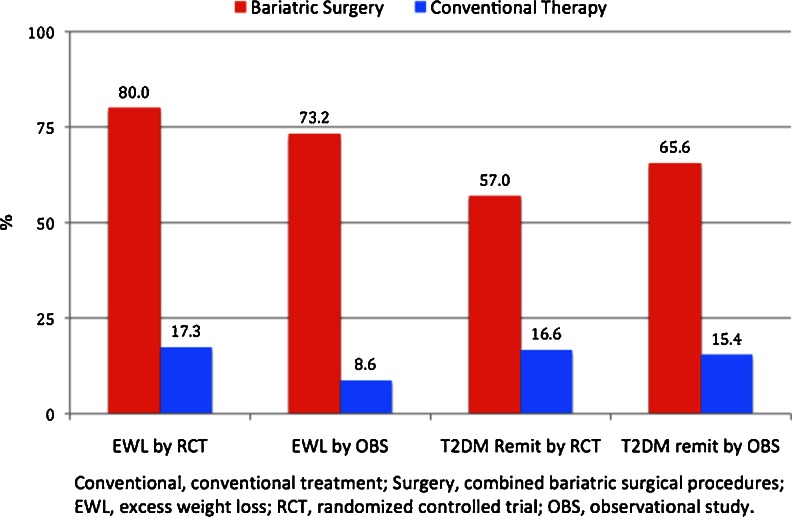
We performed a meta-analysis of weight loss and remission of type 2 diabetes mellitus (T2DM) evaluated in randomized controlled trials (RCTs) and observational studies of bariatric surgery vs conventional medical therapy. English articles published through June 10, 2013 that compared bariatric surgery with conventional therapy and included T2DM endpoints with ≥12-month follow-up were systematically reviewed. Body mass index (BMI, in kilogram per square meter), glycated hemoglobin (HbA1C, in degree), and fasting plasma glucose (FPG, in milligram per deciliter) were analyzed by calculating weighted mean differences (WMDs) and pooled standardized mean differences and associated 95 % confidence intervals (95 % CI). Aggregated T2DM remission event data were analyzed by calculating the pooled odds ratio (POR) and 95 % CI. Random effects assumptions were applied throughout; I(2) ≥ 75.0 % was considered indicative of significant heterogeneity. Systematic review identified 512 articles: 47 duplicates were removed, 446 failed inclusion criteria (i.e., n < 10 per arm, animal studies, reviews, case reports, abstracts, and kin studies). Of 19 eligible articles, two not focused on diagnosed T2DM and one with insufficient T2DM data were excluded. In the final 16 included papers, 3,076 patients (mean BMI, 40.9; age, 47.0; 72.0 % female) underwent bariatric surgery; 3,055 (39.4; 48.6, 69.0 %) received conventional or no weight-loss therapy. In bariatric surgery vs conventional therapy groups, the mean 17.3 ± 5.7 month BMI WMD was 8.3 (7.0, 9.6; p < 0.001; I(2) = 91.8), HbA(1C) was 1.1 (0.6, 1.6; p < 0.001; I(2) = 91.9), and FPG, 24.9 (15.9, 33.9; p < 0.001; I(2) = 84.8), with significant differences favoring surgery. The overall T2DM remission rate for surgery vs conventional group was 63.5 vs 15.6 % (p < 0.001). The Peto summary POR was 9.8 (6.1, 15.9); inverse variance summary POR was 15.8 (7.9, 31.4). Of the included studies, 94.0 % demonstrated a significant statistical advantage favoring surgery. In a meta-analysis of 16 studies (5 RCTs) with 6,131 patients and mean 17.3-month follow-up, bariatric surgery was significantly more effective than conventional medical therapy in achieving weight loss, HbA(1C) and FPG reduction, and diabetes remission. The odds of bariatric surgery patients reaching T2DM remission ranged from 9.8 to 15.8 times the odds of patients treated with conventional therapy.
Figures

References
-
- Sims EH, et al. Endocrine and metabolic effects of experimental obesity in man. Recent Prog Horm Res. 1973;29:457–96. - PubMed
-
- World Health Organization. Obesity and overweight—fact sheet No. 311. Updated March 2013. Accessed June 11, 2013: http://www.who.int/mediacentre/factsheets/fs311/en/index.html
-
- World Health Organization. Obesity and overweight—fact sheet no. 312. Updated March 2013. http://www.who.int/mediacentre/factsheets/fs312/en/. Accessed 11 June 2013
-
- Andersson C, van Gaal L, Caterson ID, et al. Relationship between HbA1C levels and risk of cardiovascular adverse outcomes and all-cause mortality in overweight and obese cardiovascular high-risk women and men with type 2 diabetes. Diabetologia. 2012;55(9):2348–55. doi: 10.1007/s00125-012-2584-3. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
