

Patient-reported outcomes in women with breast cancer enrolled in a dual-center, double-blind, randomized controlled trial assessing the effect of acupuncture in reducing aromatase inhibitor-induced musculoskeletal symptoms
- PMID: 24375332
- PMCID: PMC3946917
- DOI: 10.1002/cncr.28352
Patient-reported outcomes in women with breast cancer enrolled in a dual-center, double-blind, randomized controlled trial assessing the effect of acupuncture in reducing aromatase inhibitor-induced musculoskeletal symptoms
Abstract
Background: Aromatase inhibitors (AIs) have been associated with decrements in patient-reported outcomes (PROs). The objective of this study was to assess whether real acupuncture (RA), compared with sham acupuncture (SA), improves PROs in patients with breast cancer who are receiving an adjuvant AI.
Methods: Postmenopausal women with a stage 0 through III breast cancer who received an AI and had treatment-associated musculoskeletal symptoms were randomized to receive 8 weekly RA versus SA in a dual-center, randomized controlled trial. The National Surgical Adjuvant Breast and Bowel Project (NSABP) menopausal symptoms questionnaire, the Center for Epidemiological Studies Depression (CESD) scale, the Hospital Anxiety and Depression Scale (HADS), the Pittsburgh Sleep Quality Index (PSQI), the hot flash daily diary, the Hot Flash-Related Daily Interference Scale (HFRDI), and the European quality-of-life survey (EuroQol) were used to assess PROs at baseline and at 4weeks, 8 weeks, and 12 weeks.
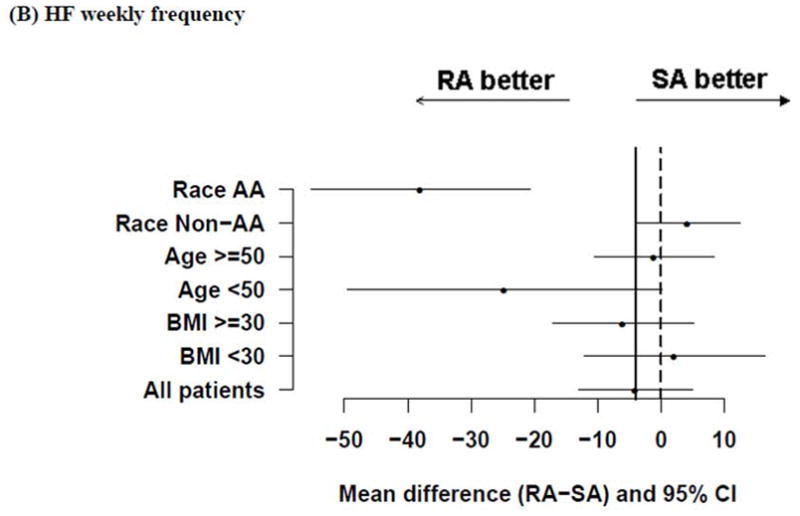
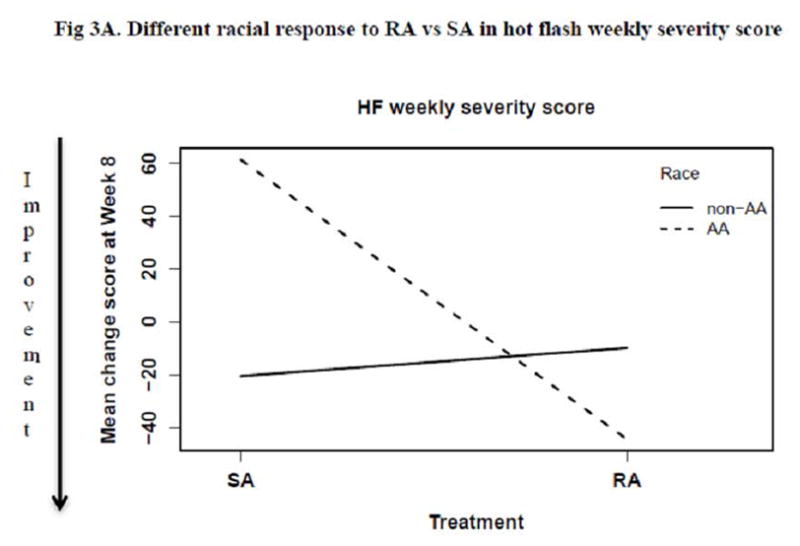
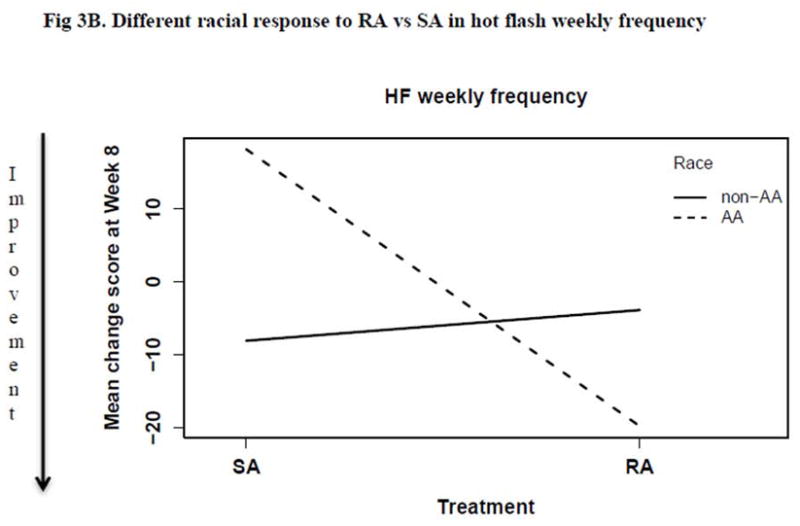
Results: The intention-to-treat analysis included 23 patients in the RA arm and 24 patients in the SA arm. There were no significant differences in baseline characteristics between the 2 groups. Compared with baseline, scores in the RA arm improved significantly at week 8 on the CESD (P = .022), hot flash severity (P = .006), hot flash frequency (P = .011), the HFRDI (P = .014), and NSABP menopausal symptoms (P = .022); scores in the SA arm improved significantly on the EuroQol (P = .022),the HFRDI (P = .043), and NSABP menopausal symptoms (P = .005). Post-hoc analysis indicated that African American patients (n = 9) benefited more from RA than SA compared with non-African American patients (n = 38) in reducing hot flash severity (P < .001) and frequency (P < .001) scores.
Conclusions: Both RA and SA were associated with improvement in PROs among patients with breast cancer who were receiving AIs, and no significant difference was detected between arms. Racial differences in response to acupuncture warrant further study.
Keywords: acupuncture; aromatase inhibitor; musculoskeletal symptoms; patient-reported outcomes.
© 2013 American Cancer Society.
Conflict of interest statement
Dr. Saranya Chumsri has consultant/advisory role in Novartis, and receives research funding from Novartis, GSK, Merck; Dr. Vered Stearns receives research funding from Pfizer, Novartis.
Figures


References
-
- Burstein HJ, et al. American Society of Clinical Oncology clinical practice guideline: update on adjuvant endocrine therapy for women with hormone receptor-positive breast cancer. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 2010;28(23):3784–96. - PMC - PubMed
-
- Morales L, et al. Acute effects of tamoxifen and third-generation aromatase inhibitors on menopausal symptoms of breast cancer patients. Anticancer Drugs. 2004;15(8):753–60. - PubMed
-
- Fallowfield L, et al. Quality of life of postmenopausal women in the Arimidex, Tamoxifen, Alone or in Combination (ATAC) Adjuvant Breast Cancer Trial. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 2004;22(21):4261–71. - PubMed
-
- Fallowfield LJ, et al. Quality of life in the intergroup exemestane study: a randomized trial of exemestane versus continued tamoxifen after 2 to 3 years of tamoxifen in postmenopausal women with primary breast cancer. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 2006;24(6):910–7. - PubMed
-
- Whelan TJ, et al. Assessment of quality of life in MA.17: a randomized, placebo-controlled trial of letrozole after 5 years of tamoxifen in postmenopausal women. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 2005;23(28):6931–40. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
