

Kidney biomarkers and differential diagnosis of patients with cirrhosis and acute kidney injury
- PMID: 24375576
- PMCID: PMC4065642
- DOI: 10.1002/hep.26980
Kidney biomarkers and differential diagnosis of patients with cirrhosis and acute kidney injury
Abstract
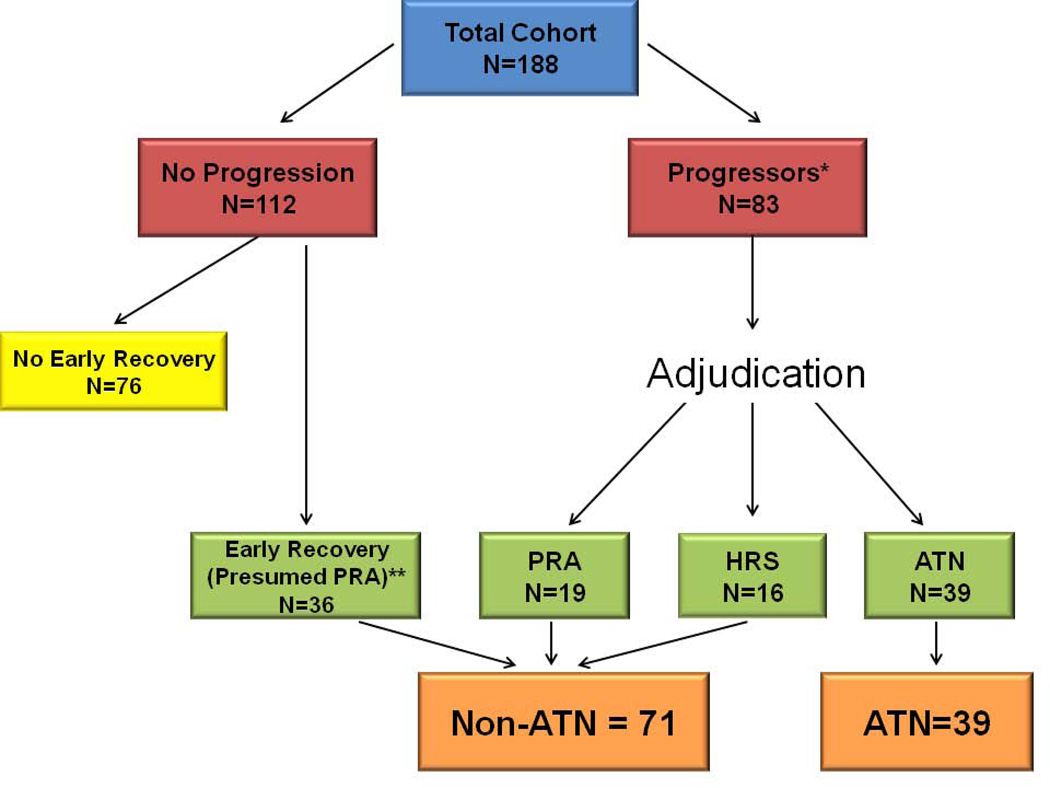
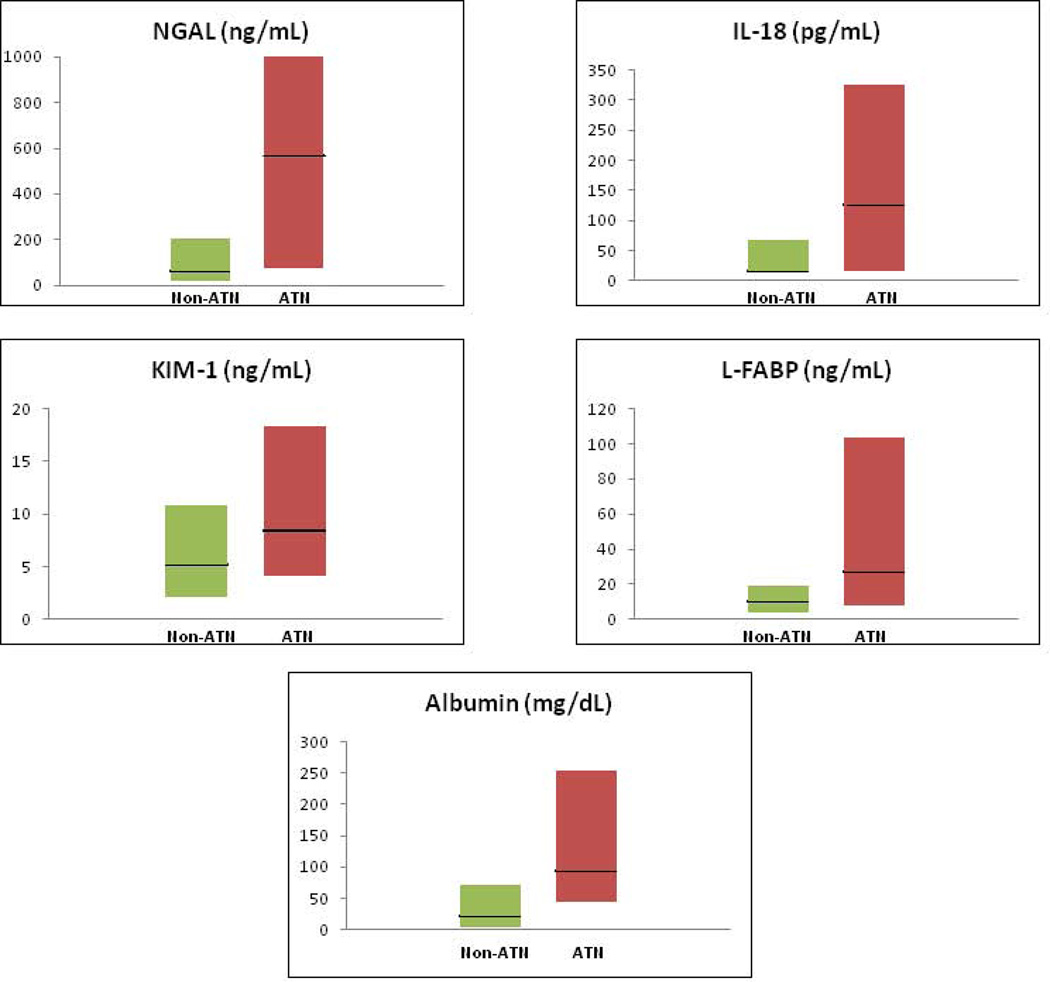
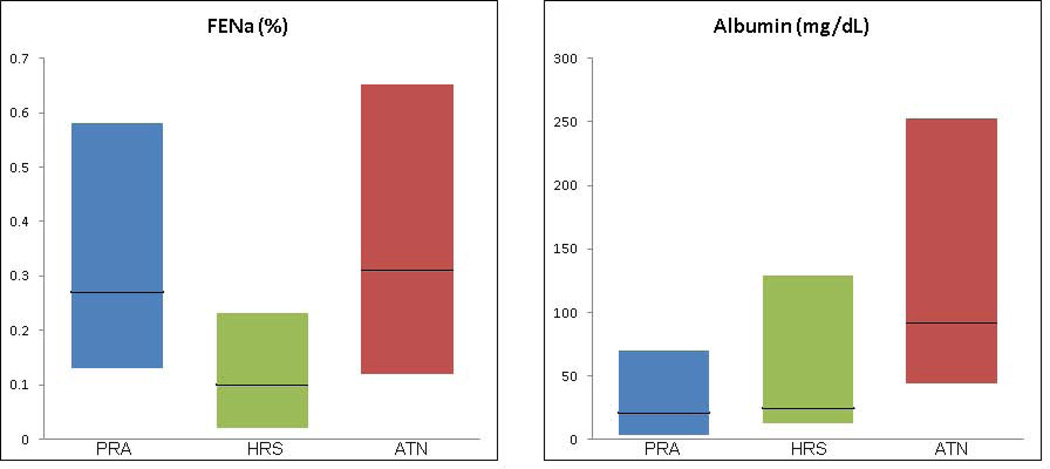
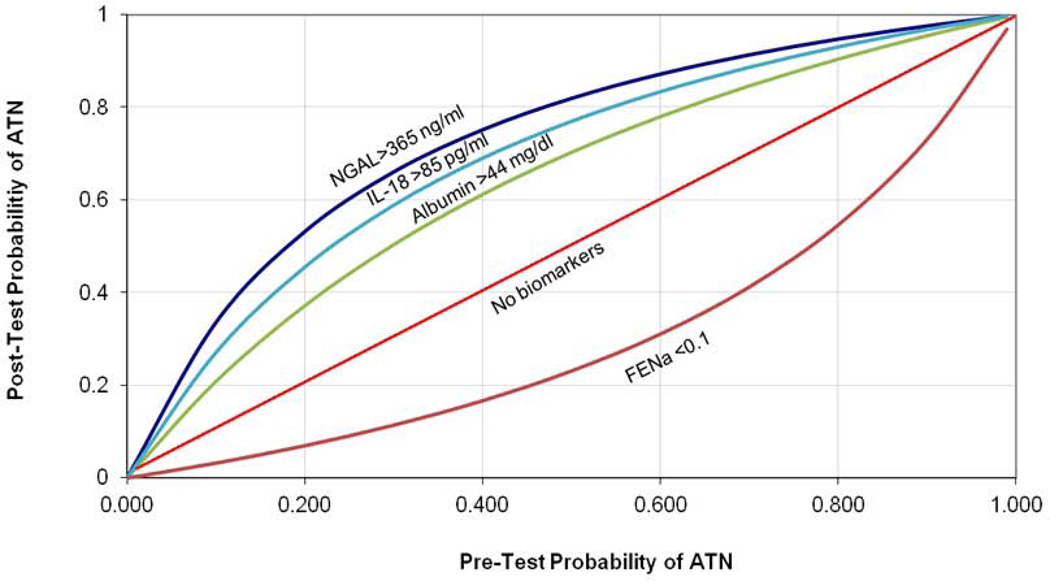
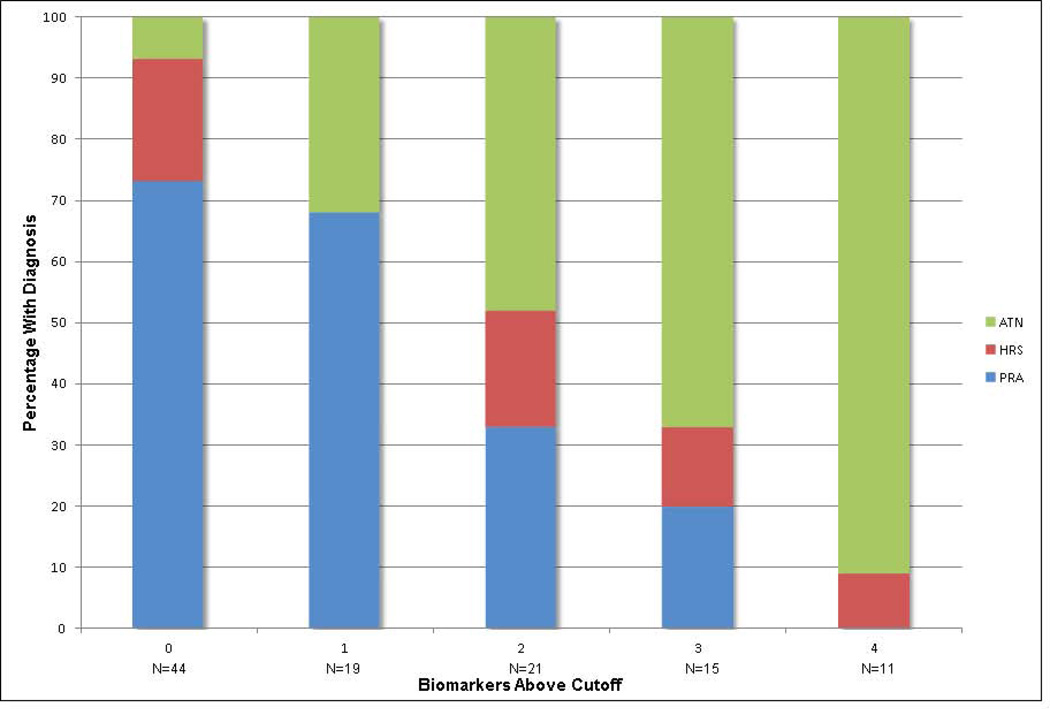
Acute kidney injury (AKI) is common in patients with cirrhosis and associated with significant mortality. The most common etiologies of AKI in this setting are prerenal azotemia (PRA), acute tubular necrosis (ATN), and hepatorenal syndrome (HRS). Accurately distinguishing the etiology of AKI is critical, as treatments differ markedly. However, establishing an accurate differential diagnosis is extremely challenging. Urinary biomarkers of kidney injury distinguish structural from functional causes of AKI and may facilitate more accurate and rapid diagnoses. We conducted a multicenter, prospective cohort study of patients with cirrhosis and AKI assessing multiple biomarkers for differential diagnosis of clinically adjudicated AKI. Patients (n = 36) whose creatinine returned to within 25% of their baseline within 48 hours were diagnosed with PRA. In addition, 76 patients with progressive AKI were diagnosed by way of blinded retrospective adjudication. Of these progressors, 39 (53%) patients were diagnosed with ATN, 19 (26%) with PRA, and 16 (22%) with HRS. Median values for neutrophil gelatinase-associated lipocalin (NGAL), interleukin-18 (IL-18), kidney injury molecule-1 (KIM-1), liver-type fatty acid binding protein (L-FABP), and albumin differed between etiologies and were significantly higher in patients adjudicated with ATN. The fractional excretion of sodium (FENa) was lowest in patients with HRS, 0.10%, but did not differ between those with PRA, 0.27%, or ATN, 0.31%, P = 0.54. The likelihood of being diagnosed with ATN increased step-wise with the number of biomarkers above optimal diagnostic cutoffs.
Conclusion: Urinary biomarkers of kidney injury are elevated in patients with cirrhosis and AKI due to ATN. Incorporating biomarkers into clinical decision making has the potential to more accurately guide treatment by establishing which patients have structural injury underlying their AKI. Further research is required to document biomarkers specific to HRS.
© 2014 by the American Association for the Study of Liver Diseases.
Figures
Comment in
-
Kidney damage biomarkers: Novel tools for the diagnostic assessment of acute kidney injury in cirrhosis.Hepatology. 2014 Aug;60(2):455-7. doi: 10.1002/hep.27063. Epub 2014 Jun 18. Hepatology. 2014. PMID: 24700173 No abstract available.
References
-
- Garcia-Tsao G, Parikh CR, Viola A. Acute kidney injury in cirrhosis. Hepatology. 2008;48:2064–2077. - PubMed
-
- Cárdenas A, Ginés P, Uriz J, Bessa X, Salmerón JM, Mas A, et al. Renal failure after upper gastrointestinal bleeding in cirrhosis: incidence, clinical course, predictive factors, and short-term prognosis. Hepatology. 2001;34(4):671–676. - PubMed
-
- Arroyo V, Fernandez J. Pathophysiological basis of albumin use in cirrhosis. Ann Hepatol. 2011;10(Suppl 1):S6–S14. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous