

Foot and ankle joint movements inside orthoses for children with spastic CP
- PMID: 24375587
- PMCID: PMC4502580
- DOI: 10.1002/jor.22567
Foot and ankle joint movements inside orthoses for children with spastic CP
Abstract
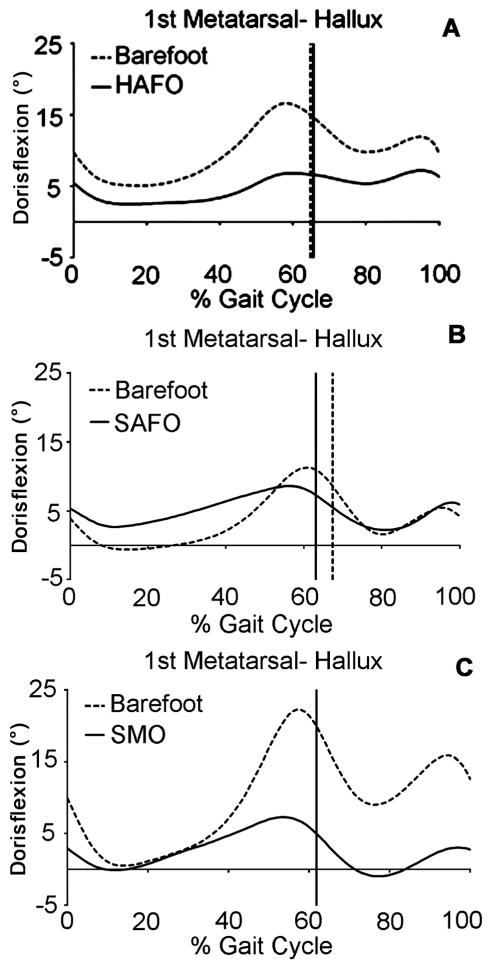
We compared the ankle joint and foot segment kinematics of pediatric cerebral palsy (CP) participants walking with and without orthoses. A six segment foot model (6SF) was used to track foot motion. Holes were cut in the study orthoses so that electromagnetic markers could be directly placed on the skin. The Hinged Ankle Foot Orthoses (HAFO) allowed a significant increase in ankle dorsiflexion as compared to the barefoot condition during gait, but significantly constrained sagittal forefoot motion and forefoot sagittal range of motion (ROM) (p < 0.01), which may be detrimental. The Solid Ankle Foot Orthoses (SAFO) constrained forefoot ROM as compared to barefoot gait (p < 0.01). The 6SF model did not confirm that the SAFO can control excessive plantarflexion for those with severe plantarflexor spasticity. The supramalleolar orthosis (SMO) significantly (p < 0.01) constrained forefoot ROM as compared to barefoot gait at the beginning and end of the stance phase, which could be detrimental. The SMO had no effects observed in the coronal plane.
Keywords: cerebral palsy; foot segment model; gait; orthoses.
© 2013 Orthopaedic Research Society. Published by Wiley Periodicals, Inc.
Figures


Similar articles
-
Long-Term Effects of Orthoses Use on the Changes of Foot and Ankle Joint Motions of Children With Spastic Cerebral Palsy.PM R. 2018 Mar;10(3):269-275. doi: 10.1016/j.pmrj.2017.08.438. Epub 2017 Sep 1. PM R. 2018. PMID: 28867667
-
Upper body movements in children with hemiplegic cerebral palsy walking with and without an ankle-foot orthosis.Clin Biomech (Bristol). 2014 Apr;29(4):387-94. doi: 10.1016/j.clinbiomech.2014.02.005. Epub 2014 Mar 5. Clin Biomech (Bristol). 2014. PMID: 24656413
-
Muscle activity in children with spastic unilateral cerebral palsy when walking with ankle-foot orthoses: an explorative study.Gait Posture. 2020 Jul;80:31-36. doi: 10.1016/j.gaitpost.2020.05.011. Epub 2020 May 23. Gait Posture. 2020. PMID: 32485421
-
The effect of tuning ankle foot orthoses-footwear combination on the gait parameters of children with cerebral palsy.Prosthet Orthot Int. 2013 Apr;37(2):95-107. doi: 10.1177/0309364612450706. Epub 2012 Jul 24. Prosthet Orthot Int. 2013. PMID: 22833518 Review.
-
Impact of Ankle-Foot Orthosis on Gait Efficiency in Ambulatory Children With Cerebral Palsy: A Systematic Review and Meta-analysis.Am J Phys Med Rehabil. 2019 Sep;98(9):759-770. doi: 10.1097/PHM.0000000000001185. Am J Phys Med Rehabil. 2019. PMID: 30920399
Cited by
-
Do research papers provide enough information on design and material used in ankle foot orthoses for children with cerebral palsy? A systematic review.J Child Orthop. 2017 Aug 1;11(4):263-271. doi: 10.1302/1863-2548.11.160256. J Child Orthop. 2017. PMID: 28904631 Free PMC article.
-
Long-term follow-up of children with a surgically treated clubfoot: Assessing the multi-segment-foot motions, dynamic plantar pressures, and functional outcomes.J Clin Orthop Trauma. 2021 Dec 30;25:101758. doi: 10.1016/j.jcot.2021.101758. eCollection 2022 Feb. J Clin Orthop Trauma. 2021. PMID: 35036311 Free PMC article.
References
-
- Davids JR. The foot and ankle in cerebral palsy. Orthop Clin North Am. 2010;41:579–593. - PubMed
-
- Davids JR, Rowan F, Davis RB. Indications for orthoses to improve gait in children with cerebral palsy. J Am Acad Orthop Surg. 2007;15:178–188. - PubMed
-
- Abel MF, Juhl GA, Vaughan CL, et al. Gait assessment of fixed ankle-foot orthoses in children with spastic diplegia. Arch Phys Med Rehabil. 1998;79:126–133. - PubMed
-
- Rethlefsen S, Kay R, Dennis S, et al. The effects of fixed and articulated ankle-foot orthoses on gait patterns in subjects with cerebral palsy. J Pediatr Orthop. 1999;19:470–474. - PubMed
-
- White H, Jenkins J, Neace WP, et al. Clinically prescribed orthoses demonstrate an increase in velocity of gait in children with cerebral palsy: a retrospective study. Dev Med Child Neurol. 2002;44:227–232. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
