

Reducing Abnormal Muscle Coactivation After Stroke Using a Myoelectric-Computer Interface: A Pilot Study
- PMID: 24376069
- PMCID: PMC4074272
- DOI: 10.1177/1545968313517751
Reducing Abnormal Muscle Coactivation After Stroke Using a Myoelectric-Computer Interface: A Pilot Study
Abstract
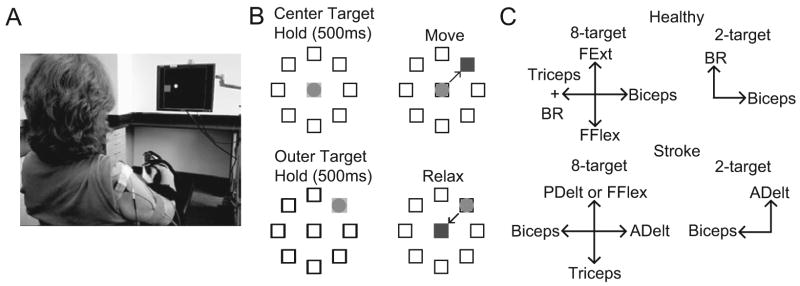
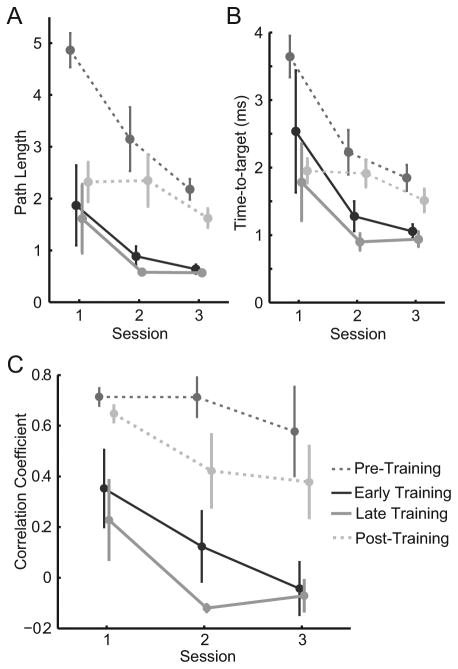
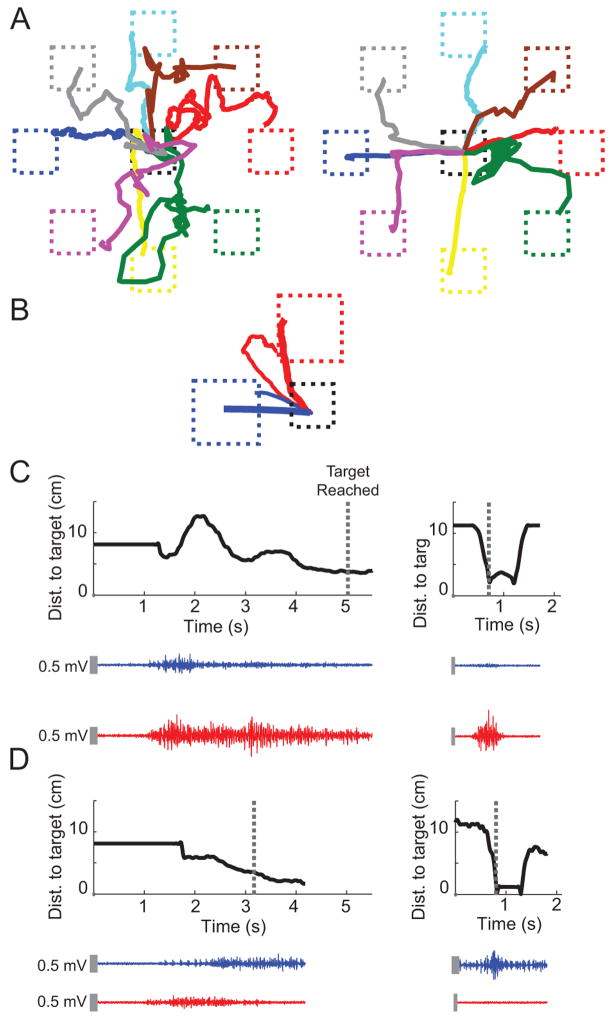
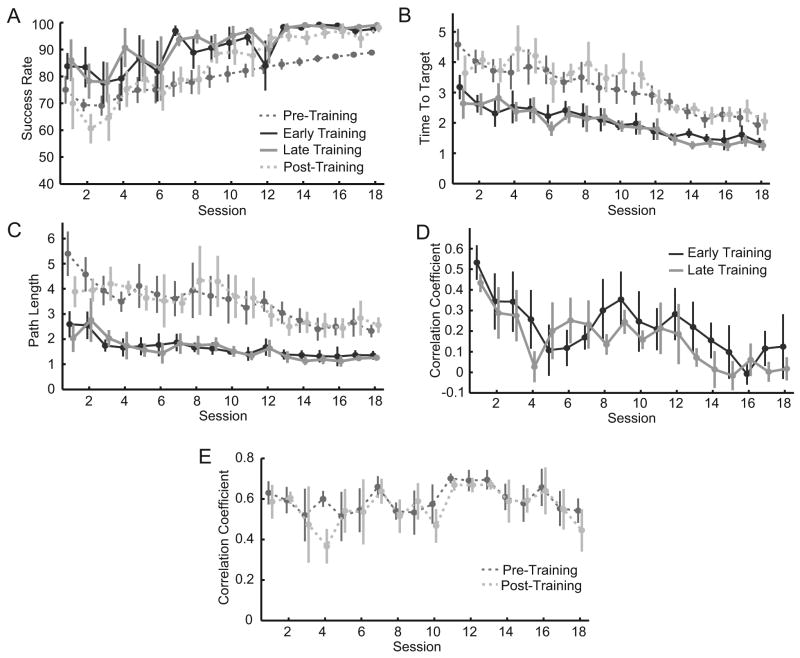
Background A significant factor in impaired movement caused by stroke is the inability to activate muscles independently. Although the pathophysiology behind this abnormal coactivation is not clear, reducing the coactivation could improve overall arm function. A myoelectric computer interface (MCI), which maps electromyographic signals to cursor movement, could be used as a treatment to help retrain muscle activation patterns. Objective To investigate the use of MCI training to reduce abnormal muscle coactivation in chronic stroke survivors. Methods A total of 5 healthy participants and 5 stroke survivors with hemiparesis participated in multiple sessions of MCI training. The level of arm impairment in stroke survivors was assessed using the upper-extremity portion of the Fugl-Meyer Motor Assessment (FMA-UE). Participants performed isometric activations of up to 5 muscles. Activation of each muscle was mapped to different directions of cursor movement. The MCI specifically targeted 1 pair of muscles in each participant for reduction of coactivation. Results Both healthy participants and stroke survivors learned to reduce abnormal coactivation of the targeted muscles with MCI training. Out of 5 stroke survivors, 3 exhibited objective reduction in arm impairment as well (improvement in FMA-UE of 3 points in each of these patients). Conclusions These results suggest that the MCI was an effective tool in directly retraining muscle activation patterns following stroke.
Keywords: EMG; arm; coactivation; muscles; rehabilitation; stroke; synergies.
© The Author(s) 2013.
Figures
References
-
- Kwakkel G, Kollen BJ, van der Grond J, Prevo AJH. Probability of regaining dexterity in the flaccid upper limb. Stroke. 2003;34:2181–2186. - PubMed
-
- Dewald J, Pope PS, Given JD, Buchanan TS, Rymer WZ. Abnormal muscle coactivation patterns during isometric torque generation at the elbow and shoulder in hemiparetic subjects. Brain. 1995;118:495. - PubMed
-
- Beer RF, Dewald JP, Rymer WZ. Deficits in the coordination of multijoint arm movements in patients with hemiparesis: evidence for disturbed control of limb dynamics. Exp Brain Res. 2000;131:305–319. - PubMed
-
- Dewald J, Beer RF. Abnormal joint torque patterns in the paretic upper limb of subjects with hemiparesis. Muscle Nerve. 2001;24:273–283. - PubMed
-
- Zackowski KM, Dromerick AW, Sahrmann SA, Thach WT, Bastian AJ. How do strength, sensation, spasticity and joint individuation relate to the reaching deficits of people with chronic hemiparesis? Brain. 2004;127:1035–1046. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
