

Variations among primary care physicians in exercise advice, imaging, and analgesics for musculoskeletal pain: results from a factorial experiment
- PMID: 24376249
- PMCID: PMC4067704
- DOI: 10.1002/acr.22143
Variations among primary care physicians in exercise advice, imaging, and analgesics for musculoskeletal pain: results from a factorial experiment
Abstract
Objective: To examine whether medical decisions regarding evaluation and management of musculoskeletal pain conditions varied systematically by characteristics of the patient or provider.
Methods: We conducted a balanced factorial experiment among primary care physicians in the US. Physicians (n = 192) viewed 2 videos of different patients (actors) presenting with pain: undiagnosed sciatica symptoms or diagnosed knee osteoarthritis. Systematic variations in patient gender, socioeconomic status, and race and physician gender and experience (<20 versus ≥20 years in practice) permitted estimation of unconfounded effects. Analysis of variance was used to evaluate associations between patient or provider attributes and clinical decisions. Quality of decisions was defined based on the current recommendations of the American College of Rheumatology, American Pain Society, and clinical expert consensus.
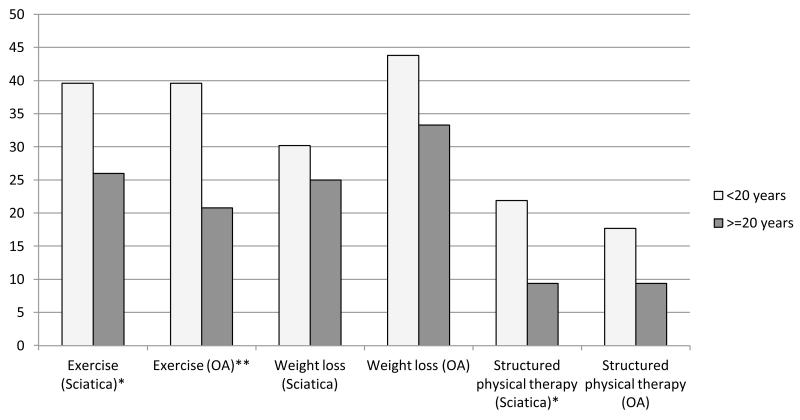
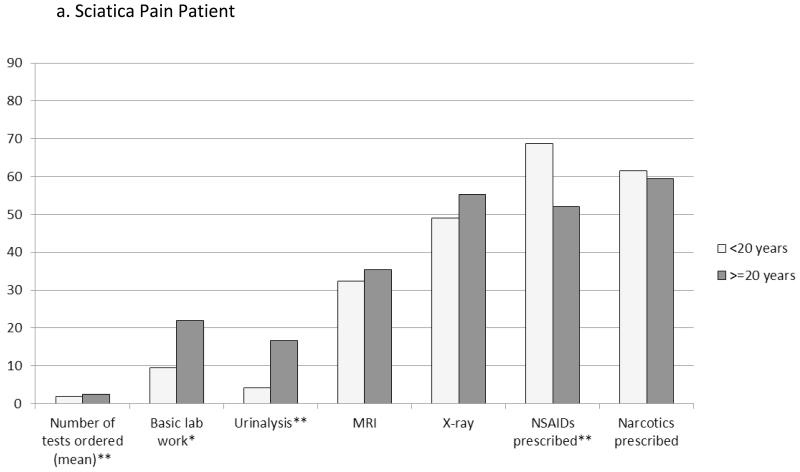
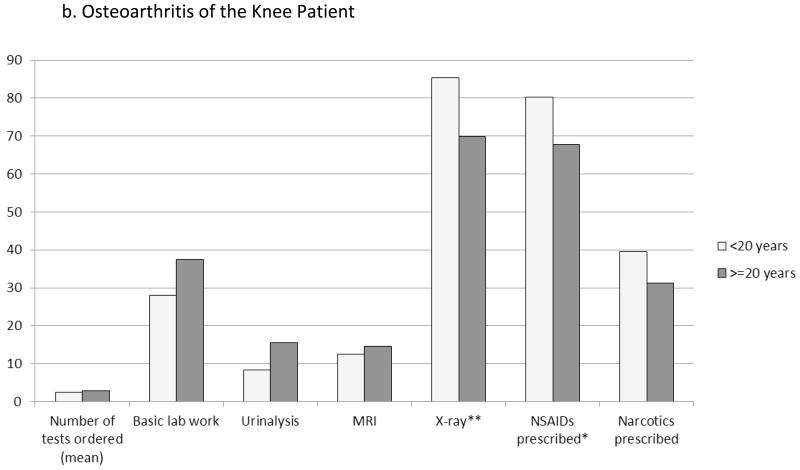
Results: Despite current recommendations, less than one-third of physicians would provide exercise advice (30.2% for osteoarthritis and 32.8% for sciatica). Physicians with fewer years in practice were more likely to provide advice on lifestyle changes, particularly exercise (P ≤ 0.01), and to prescribe nonsteroidal antiinflammatory drugs for pain relief, both of which were appropriate and consistent with current recommendations for care. Newer physicians ordered fewer tests, particularly basic laboratory investigations or urinalysis. Test ordering decreased as organizational emphasis on business or profits increased. Patient factors and physician gender had no consistent effects on pain evaluation or treatment.
Conclusion: Physician education on disease management recommendations regarding exercise and analgesics and implementation of quality measures may be useful, particularly for physicians with more years in practice.
Copyright © 2014 by the American College of Rheumatology.
Figures
References
-
- Institute of Medicine . Relieving pain in America: a blueprint for transforming prevention, care, education, and research. Washington, DC: 2011. - PubMed
-
- Pizzo PA, Clark NM. Alleviating suffering 101--pain relief in the United States. New England Journal of Medicine. 2012;366(3):197–9. - PubMed
-
- Hochberg MC, Altman RD, April KT, Benkhalti M, Guyatt G, McGowan J, et al. American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee. Arthritis care & research. 2012;64(4):465–74. - PubMed
-
- Green CR, Wheeler JR, LaPorte F. Clinical decision making in pain management: Contributions of physician and patient characteristics to variations in practice. The Journal of Pain: Official Journal of the American Pain Society. 2003;4(1):29–39. - PubMed
-
- Tamayo-Sarver JH, Dawson NV, Hinze SW, Cydulka RK, Wigton RS, Albert JM, et al. The effect of race/ethnicity and desirable social characteristics on physicians’ decisions to prescribe opioid analgesics. Academic Emergency Medicine: Official Journal of the Society for Academic Emergency Medicine. 2003;10(11):1239–48. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
