

The role of drug-induced sleep endoscopy in the diagnosis and management of obstructive sleep apnoea syndrome: our personal experience
- PMID: 24376297
- PMCID: PMC3870452
The role of drug-induced sleep endoscopy in the diagnosis and management of obstructive sleep apnoea syndrome: our personal experience
Abstract
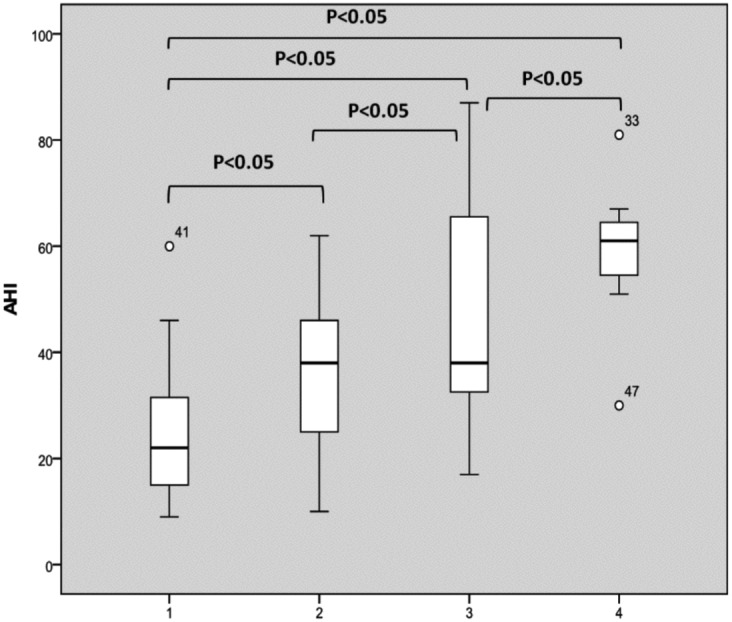
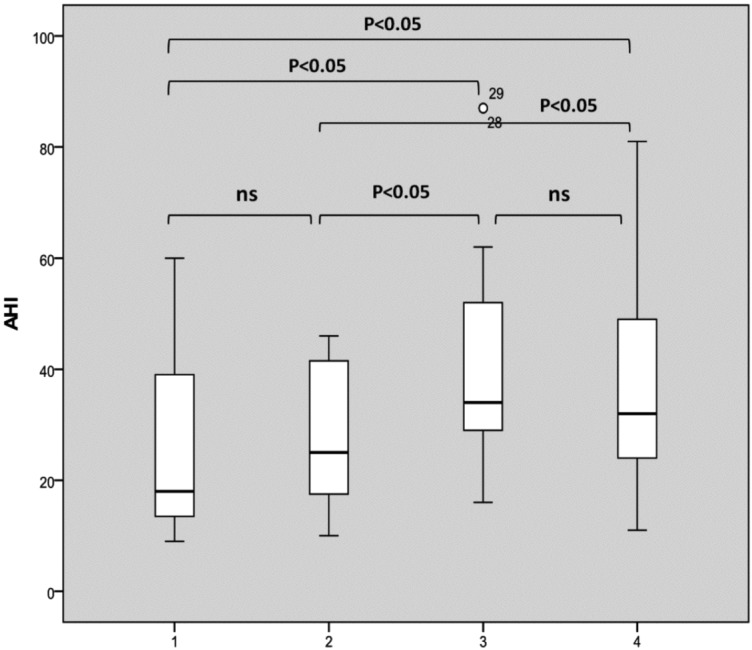
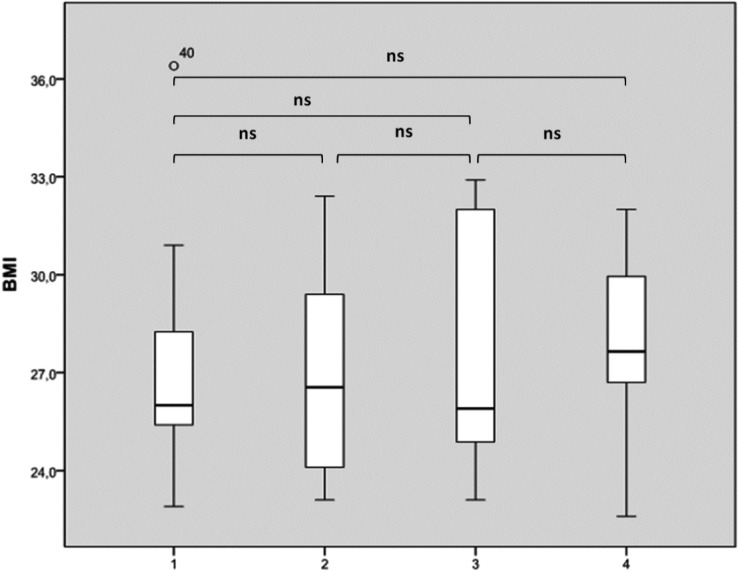
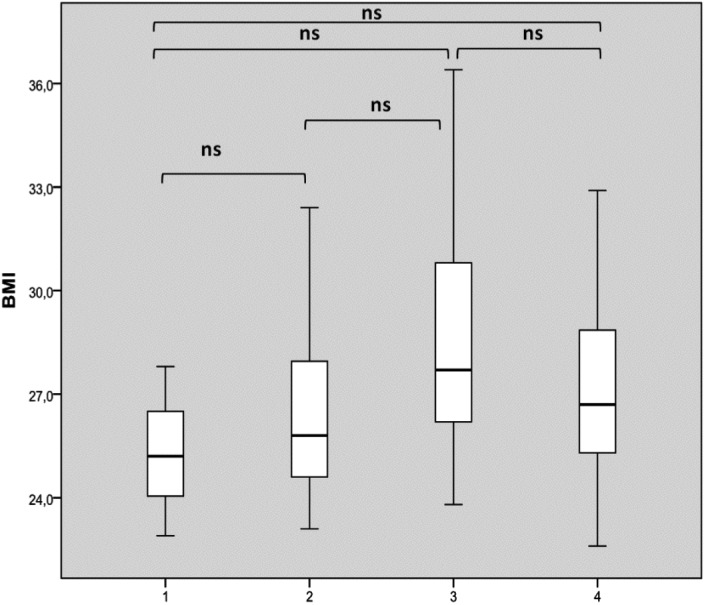
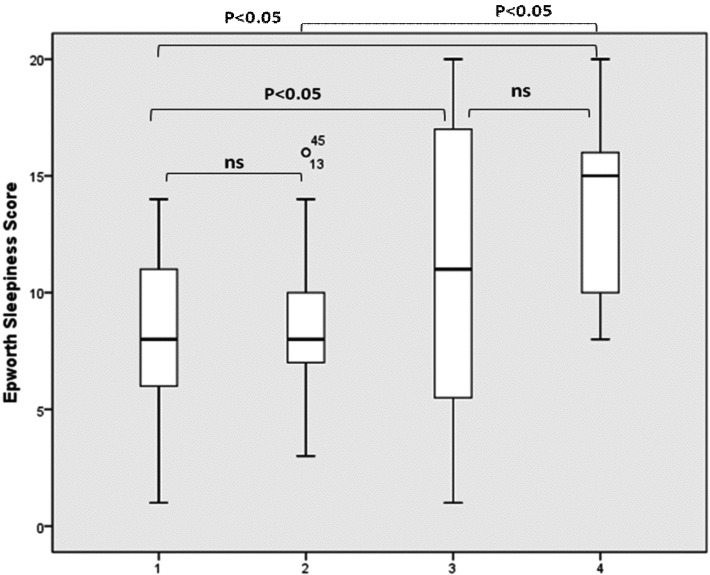
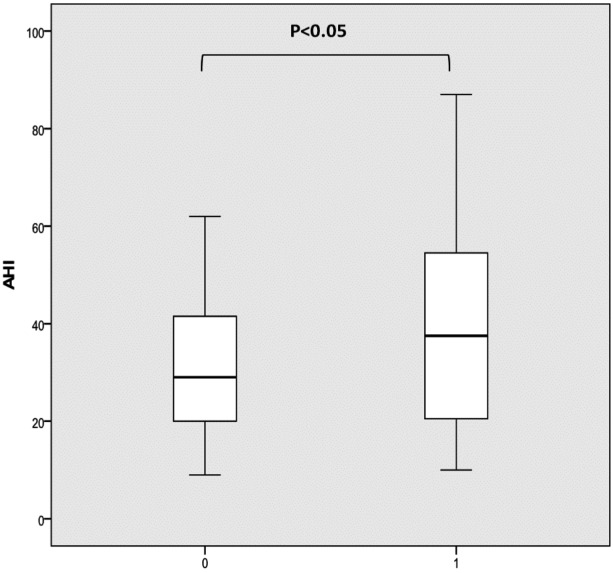
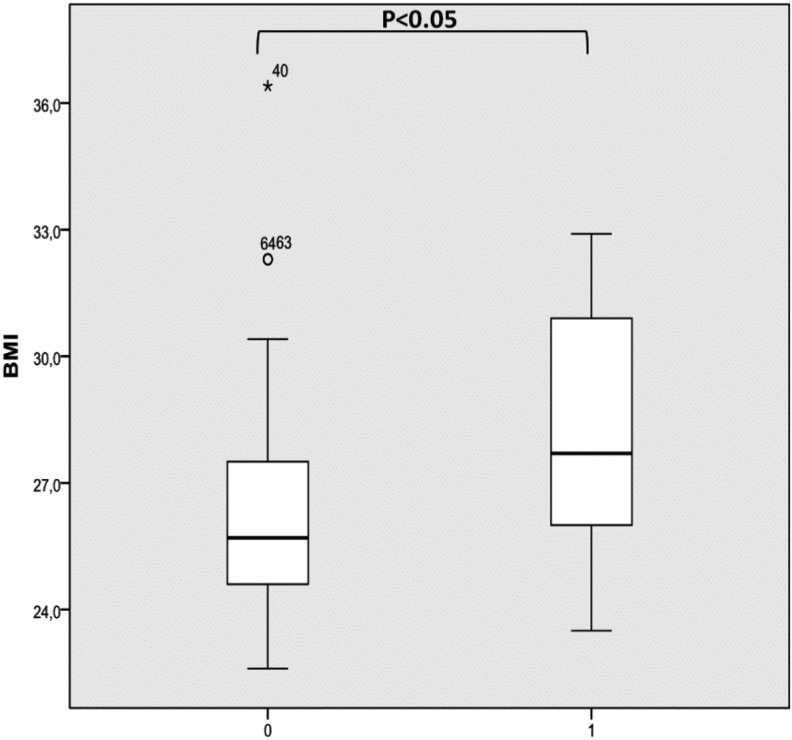
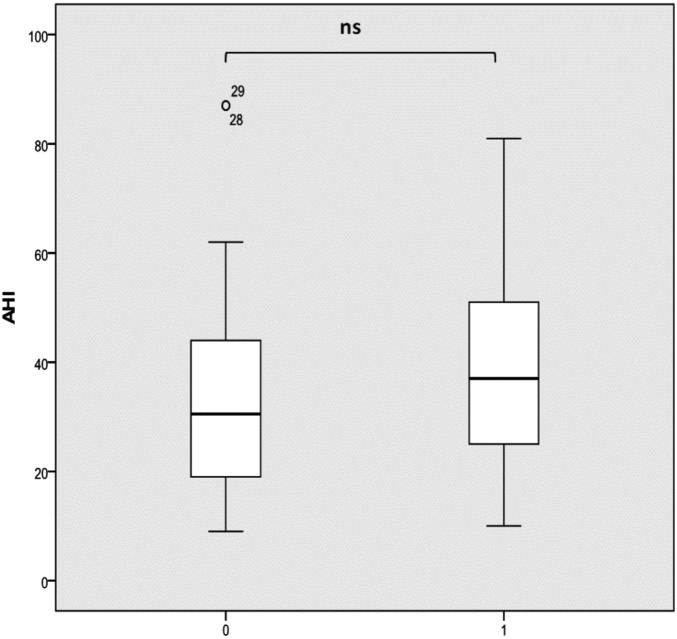
Nowadays, drug-induced sleep endoscopy (DISE) is performed widely and its validity and reliability has been demonstrated by several studies; in fact, it provides clinical information not available by routine clinical inspection alone. Its safety and utility are promising, but still needs to be improved to reach the level of excellence expected of gold standard tests used in clinical practice. Our study compares the results of clinical and diagnostic evaluation with those of sleep endoscopy, evaluating the correlation between clinical indexes of routine clinical diagnosis and sites of obstruction in terms of number of sites involved, entity of obstruction and pattern of closure. This study consists in a longitudinal prospective evaluation of 138 patients who successfully underwent sleep endoscopy at our institution. Patients were induced to sleep with a low dose of midazolam followed by titration with propofol. Sedation level was monitored using bispectral index monitoring. Our results suggest that the multilevel complete collapse was statistically significantly associated with higher apnoea hypopnea index values. By including partial sites of obstruction greater than 50%, our results also suggest that multilevel collapse remains statistically and significantly associated with higher apnoea hypopnoea index values. Analyzing BMI distribution based on number of sites with complete and partial obstruction there was no significant difference. Finally, analyzing Epworth Sleepiness Score distribution based on number of sites with complete obstruction, there was a statistically significant difference between patients with 3-4 sites of obstruction compared to those with two sites or uni-level obstruction. In conclusion, our data suggest that DISE is safe, easy to perform, valid and reliable, as previously reported. Furthermore, we found a good correlation between DISE findings and clinical characteristics such as AHI and EPS. Consequently, adequate assessment by DISE of all sites of obstruction is very important, not only in patients with low-moderate AHI and EPS, but also in patients with a high AHI or/and high EPS, in particular to plan multilevel surgery that in these latter situations is more demanding since success may be harder to achieve.
Attualmente, la sleep endoscopy indotta per via farmacologica (DISE) è ampiamente eseguita e la validità ed affidabilità di tale metodica sono state dimostrate in numerosi studi. La sua sicurezza e utilità sono promettenti, tuttavia, tale esame necessita di essere migliorato per raggiungere il livello di eccellenza tipico di un test gold standard utilizzato nella pratica clinica. Obiettivo del nostro studio è stato paragonare i risultati della valutazione clinica e diagnostica tradizionale con quelli della sleep endoscopy, mettendo a confronto i parametri clinici con i siti di ostruzione, ed in particolare prendendo in considerazione il numero di siti implicati, il livello di ostruzione e il pattern di chiusura. In questo studio abbiamo effettuato una valutazione prospettica longitudinale di 138 pazienti che sono stati sottoposti a sleep endoscopy con induzione farmacologica del sonno presso la nostra clinica. Ai pazienti è stato indotto il sonno mediante un basso dosaggio di propofol seguito da una somministrazione di boli progressivi. La profondità della sedazione è stata monitorata mediante il monitoraggio BIS. Sulla base dei risultati ottenuti è stato possibile stabilire che l'ostruzione completa multilivello si associa in modo statisticamente significativo ad un indice più elevato di apnea/ipopnea (AHI). Includendo nell'analisi anche i siti di ostruzione parziale con chiusura > del 50% abbiamo potuto dimostrare che l'associazione fra il collasso multilivello ed un valore di indice apnea/ipopnea più elevato rimane statisticamente significativa. Per quanto riguarda il BMI invece non sono state riscontrate correlazioni significative con il numero di siti di ostruzione completi o parziali. Infine, analizzando la scala della sonnolenza di Epworth e correlandola con il numero di siti con ostruzione completa abbiamo trovato una differenza statisticamente significativa tra i paziente con 3-4 siti di ostruzione rispetto ai pazienti con 2 o 1 livello di ostruzione. In conclusione, i nostri dati suggeriscono che la sleep endoscopy indotta per via farmacologica (DISE) costituisce una procedura sicura, di facile esecuzione, valida ed affidabile, come già descritto in altri studi. Inoltre abbiamo dimostrato una buona correlazione e coerenza tra i risultati della sleep endoscopy e gli indici di AHI e di Epworth. Concludendo riteniamo che un'adeguata valutazione dei siti di ostruzione mediante sleep endoscopy sia molto importante non solo nei pazienti con AHI ed indice di Epworth lieve/moderato, ma anche in quelli con AHI e/o indice di Epworth elevati, soprattutto nella pianificazione di una chirurgia multilivello che in questi casi è più impegnativa con un indice di successo più difficile da raggiungere.
Keywords: AHI; BMI; Drug-induced sleep endoscopy; EPS; Obstructive sleep apnoea syndrome.
Figures
References
-
- Croft CB, Pringle M. Sleep nasendoscopy: a technique of assessment in snoring and obstructive sleep apnoea. Clin Otolaryngol Allied Sci. 1991;16:504–509. - PubMed
-
- Eichler C, Sommer JU, Stuck BA, et al. Does drug-induced sleep endoscopy change the treatment concept of patients with snoring and obstructive sleep apnea? Sleep Breath. 2013;17:63–68. - PubMed
-
- Hong SD, Dhong HJ, Kim HY, et al. Change of obstruction level during drug-induced sleep endoscopy (DISE) according to sedation depth in obstructive sleep apnea. Laryngoscope. 2013 Aug 05; doi: 10.1002/lary.24045. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical