

Development of a multimorbidity illness perceptions scale (MULTIPleS)
- PMID: 24376504
- PMCID: PMC3869652
- DOI: 10.1371/journal.pone.0081852
Development of a multimorbidity illness perceptions scale (MULTIPleS)
Abstract
Background: Illness perceptions are beliefs about the cause, nature and management of illness, which enable patients to make sense of their conditions. These perceptions can predict adjustment and quality of life in patients with single conditions. However, multimorbidity (i.e. patients with multiple long-term conditions) is increasingly prevalent and a key challenge for future health care delivery. The objective of this research was to develop a valid and reliable measure of illness perceptions for multimorbid patients.
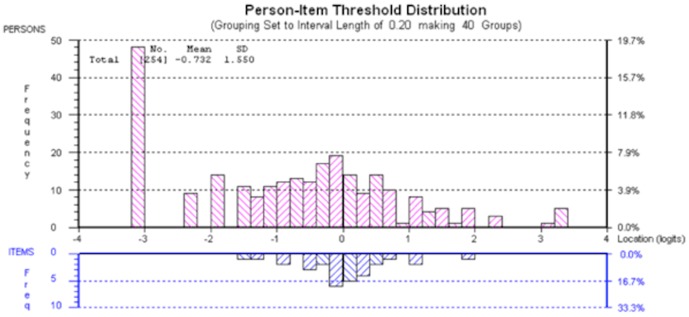
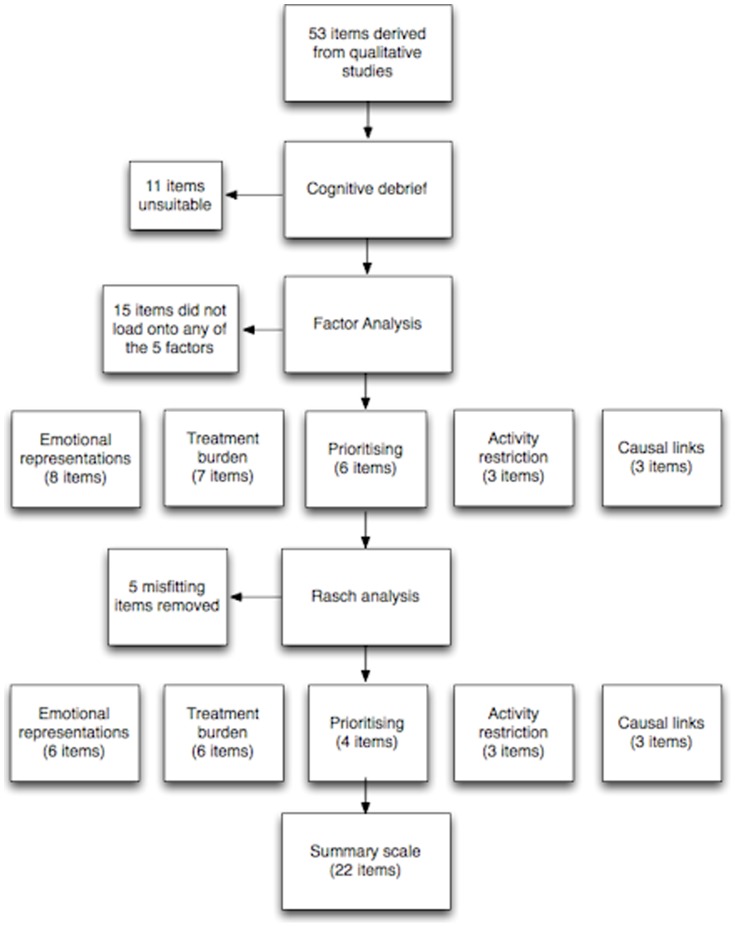
Methods: Candidate items were derived from previous qualitative research with multimorbid patients. Questionnaires were posted to 1500 patients with two or more exemplar long-term conditions (depression, diabetes, osteoarthritis, coronary heart disease and chronic obstructive pulmonary disease). Data were analysed using factor analysis and Rasch analysis. Rasch analysis is a modern psychometric technique for deriving unidimensional and intervally-scaled questionnaires.
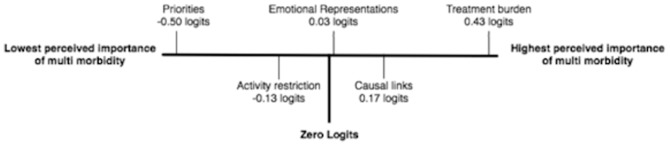
Results: Questionnaires from 490 eligible patients (32.6% response) were returned. Exploratory factor analysis revealed five potential subscales 'Emotional representations', 'Treatment burden', 'Prioritising conditions', 'Causal links' and 'Activity limitations'. Rasch analysis led to further item reduction and the generation of a summary scale comprising of items from all scales. All scales were unidimensional and free from differential item functioning or local independence of items. All scales were reliable, but for each subscale there were a number of patients who scored at the floor of the scale.
Conclusions: The MULTIPleS measure consists of five individual subscales and a 22-item summary scale that measures the perceived impact of multimorbidity. All scales showed good fit to the Rasch model and preliminary evidence of reliability and validity. A number of patients scored at floor of each subscale, which may reflect variation in the perception of multimorbidity. The MULTIPleS measure will facilitate research into the impact of illness perceptions on adjustment, clinical outcomes, quality of life, and costs in patients with multimorbidity.
Conflict of interest statement
Figures
References
-
- Wolff JL, Starfield B, Anderson G (2002) Prevalence, expenditures and complications of multiple chronic conditions in the elderly. Archives of Internal medicine 162: 2269–2276. - PubMed
-
- van den Akker M, Buntinx F, Metsemakers JFM, Roos S, Knottnerus JA (1998) Multimorbidity in general practice: Prevalence, incidence, and determinants of co-occurring chronic and recurrent diseases. Journal of Clinical Epidemiology 51: 367–375. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
