

Proof of the concept to use a malignant B cell line drug screen strategy for identification and weight of melphalan resistance genes in multiple myeloma
- PMID: 24376673
- PMCID: PMC3869769
- DOI: 10.1371/journal.pone.0083252
Proof of the concept to use a malignant B cell line drug screen strategy for identification and weight of melphalan resistance genes in multiple myeloma
Abstract
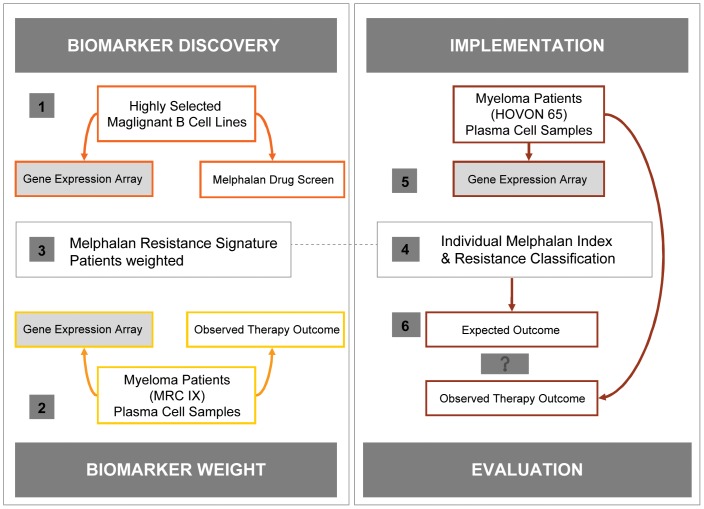
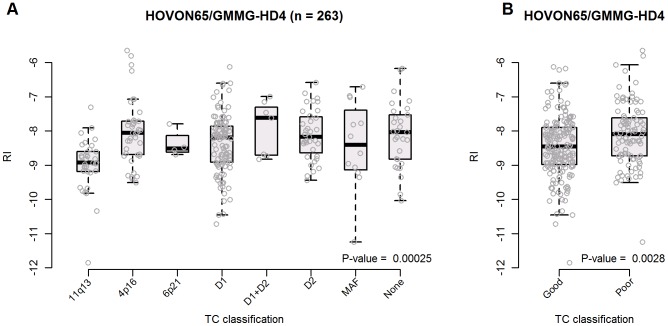
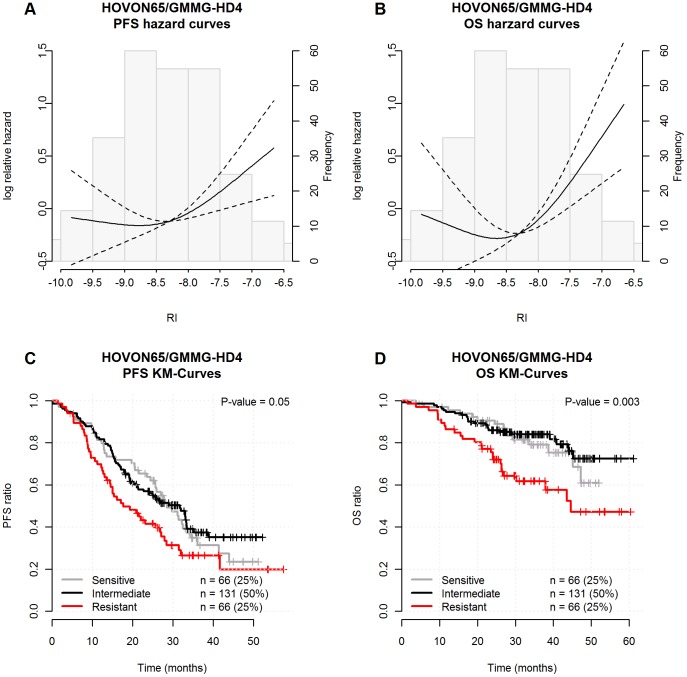
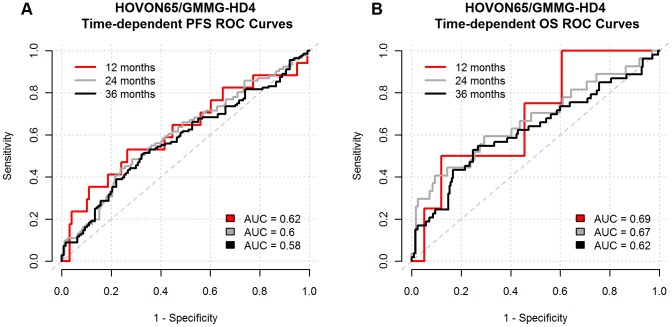
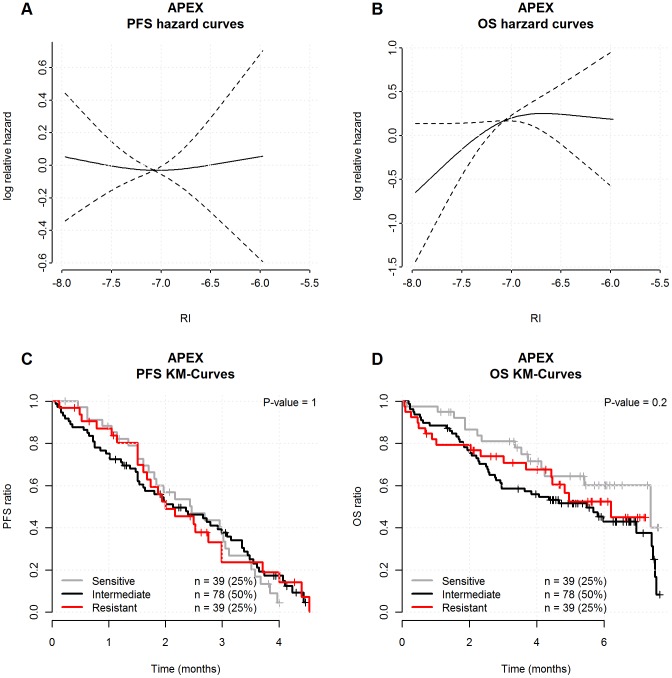
In a conceptual study of drug resistance we have used a preclinical model of malignant B-cell lines by combining drug induced growth inhibition and gene expression profiling. In the current report a melphalan resistance profile of 19 genes were weighted by microarray data from the MRC Myeloma IX trial and time to progression following high dose melphalan, to generate an individual melphalan resistance index. The resistance index was subsequently validated in the HOVON65/GMMG-HD4 trial data set to prove the concept. Biologically, the assigned resistance indices were differentially distributed among translocations and cyclin D expression classes. Clinically, the 25% most melphalan resistant, the intermediate 50% and the 25% most sensitive patients had a median progression free survival of 18, 32 and 28 months, respectively (log-rank P-value = 0.05). Furthermore, the median overall survival was 45 months for the resistant group and not reached for the intermediate and sensitive groups (log-rank P-value = 0.003) following 38 months median observation. In a multivariate analysis, correcting for age, sex and ISS-staging, we found a high resistance index to be an independent variable associated with inferior progression free survival and overall survival. This study provides clinical proof of concept to use in vitro drug screen for identification of melphalan resistance gene signatures for future functional analysis.
Conflict of interest statement
Figures
References
-
- Storm HH, Klint A, Tryggvadóttir L, Gislum M, Engholm G, et al. (2010) Trends in the survival of patients diagnosed with malignant neoplasms of lymphoid, haematopoietic, and related tissue in the Nordic countries 1964-2003 followed up to the end of 2006. Acta Oncol 49: 694–712. - PubMed
-
- Palumbo A, Bringhen S, Ludwig H, Dimopoulos MA, Bladé J, et al. (2011) Personalized therapy in multiple myeloma according to patient age and vulnerability: a report of the European Myeloma Network (EMN). Blood 118: 4519–4529. - PubMed
-
- Greipp PR, San Miguel J, Durie BG, Crowley JJ, Barlogie B, et al. (2005) International staging system for multiple myeloma. J Clin Oncol 23: 3412–3420. Epub 2005 Apr 4. Erratum (2005) J Clin Oncol 23: 6281. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
