

Dosimetric and physical comparison of IMRT and CyberKnife plans in the treatment of localized prostate cancer
- PMID: 24376947
- PMCID: PMC3863154
- DOI: 10.1016/j.rpor.2010.10.003
Dosimetric and physical comparison of IMRT and CyberKnife plans in the treatment of localized prostate cancer
Abstract
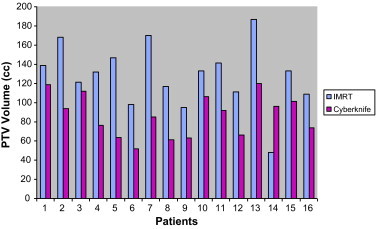
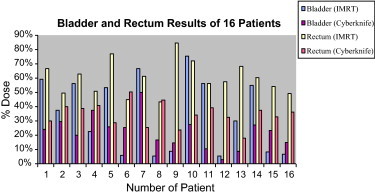
Aim: The aim of our study was the dosimetric and physical evaluation of the CK and IMRT treatment plans for 16 patients with localized prostate cancer.
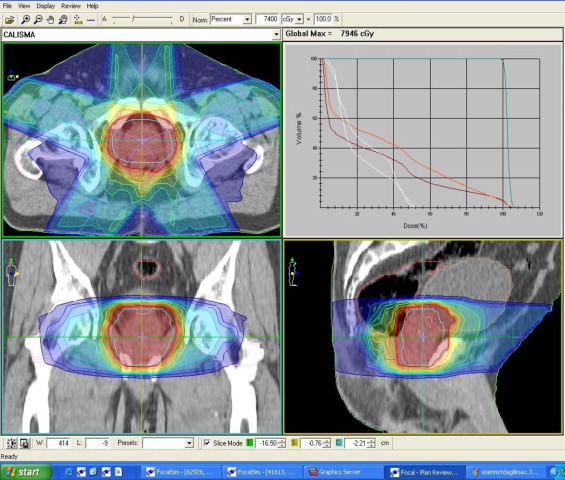
Background: Intensity modulated radiation therapy (IMRT) is one of the recent technical advances in radiotherapy. The prostate is a well suited site to be treated with IMRT. The challenge of accurately delivering the IMRT needs to be supported by new advances such as image-guidance and four-dimensional computed conformal radiation therapy (4DCRT) tomography. CyberKnife (CK) provides real time orthogonal X-ray imaging of the patient during treatment course to follow gold fiducials installed into the prostate and to achieve motion correlation between online acquired X-ray imaging and digital reconstructed radiographs (DRRs) which are obtained from planning computed tomography images by translating and rotating the treatment table in five directions.
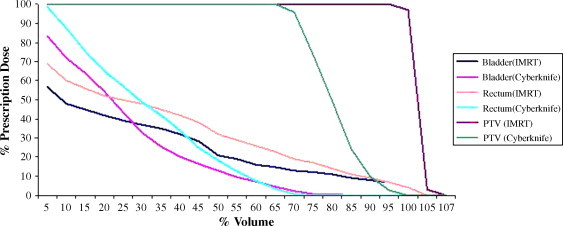
Methods and materials: Sixteen IMRT and CK plans were performed to be compared in terms of conformity (CI), heterogeneity indices (HI), percentage doses of 100% (V100), 66% (V66), 50% (V50), 33% (V33) and 10% (V10) volumes of the bladder and rectum. Dose-volume histograms for target and critical organs, (CI) and indices (HI) and isodose lines were analyzed to evaluate the treatment plans.
Results: Statistically significant differences in the percentage rectal doses delivered to V10, V33, and V50 of the rectum were detected in favor of the CK plans (p values; <0.001, <0.001 and 0.019, respectively). The percentage doses for V66 and V100 of the rectum were larger in CK plans (13%, 2% in IMRT and 21%, 3% in CK plans, respectively). Percentage bladder doses for V10 and V33 were significantly lower in CK plans [96% in IMRT vs 48% in CK (p < 0.001) and 34% in IMRT vs 24% in CK (p = 0.047)]. Lower percentage doses were observed for V50, V66 of the bladder for the IMRT. They were 5.4% and 3.45% for IMRT and 13.4% and 8.05% for CK, respectively. Median CI of planning target volume (PTV) for IMRT and CK plans were 0.94 and 1.23, respectively (p < 0.001).
Conclusion: Both systems have a very good ability to create highly conformal volumetric dose distributions. Median HI of PTV for IMRT and CK plans were 1.08 and 1.33, respectively (p < 0.001).
Keywords: CyberKnife; IMRT; Prostate; Radiosurgery.
Figures

References
-
- Ashman Jonathan B., Zelefsky Micheal J., Hunt Margie S., Leibel Steven A., Fuks Zvi. Whole pelvic radiotherapy for prostate cancer using 3D conformal and intensity-modulated radiotherapy. Int J Radiat Oncol Biol Phys. 2005;63(3):765–771. - PubMed
-
- Luxton Gary, Hancock Steven L., Boyer Arthur L. Dosimetry and radiobiological model comparison of IMRT and 3D conformal radiotherapy in treatment of carcinoma of the prostate. Int J Radiat Oncol Biol Phys. 2004;59(1):267–284. - PubMed
-
- Vlachaki Maria T., Teslow Terrance N., Amosson Chad, Uy Nathan W., Ahmad Salahuddin. IMRT versus conventional 3DCRT on prostate and normal tissue dosimetry using an endorectal balloon for prostate immobilization. Med Dosim. 2005;30(2):69–75. - PubMed
-
- James H.V., Scrase C.D., Poynter A.J. Practical experience with intensity-modulated radiotherapy. Br J Radiol. 2004;77:3–14. - PubMed
-
- Kara Bucci M., Bevan Alison, Roach Mack., III Advances in radiation therapy: conventional to 3D, to IMRT, to 4D, and beyond. CA Cancer J Clin. 2005;55:117–134. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
