

Comparison of dose distributions and organs at risk (OAR) doses in conventional tangential technique (CTT) and IMRT plans with different numbers of beam in left-sided breast cancer
- PMID: 24376964
- PMCID: PMC3863158
- DOI: 10.1016/j.rpor.2011.02.001
Comparison of dose distributions and organs at risk (OAR) doses in conventional tangential technique (CTT) and IMRT plans with different numbers of beam in left-sided breast cancer
Abstract
Aim: Our aim was to improve dose distribution to the left breast and to determine the dose received by the ipsilateral lung, heart, contralateral lung and contralateral breast during primary left-sided breast irradiation by using intensity modulated radiotherapy (IMRT) techniques compared to conventional tangential techniques (CTT). At the same time, different beams of IMRT plans were compared to each other in respect to CI, HI and organs at risk (OAR) dose.
Background: Conventional early breast cancer treatment consists of lumpectomy followed by whole breast radiation therapy. CTT is a traditional method used for whole breast radiotherapy and includes standard wedged tangents (two opposed wedged tangential photon beams). The IMRT technique has been widely used for many treatment sites, allowing both improved sparing of normal tissues and more conformal dose distributions. IMRT is a new technique for whole breast radiotherapy. IMRT is used to improve conformity and homogeneity and used to reduce OAR doses.
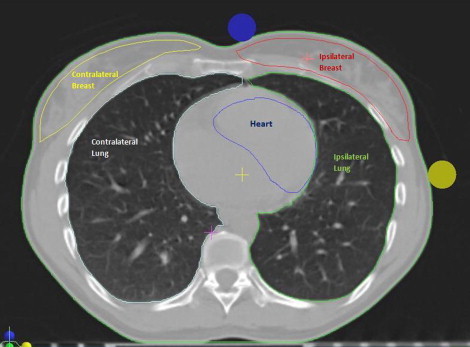
Materials and methods: Thirty patients with left-sided breast carcinoma were treated between 2005 and 2008 using 6, 18 or mixed 6/18 MV photons for primary breast irradiation following breast conserving surgery (BCS). The clinical target volume [CTV] was contoured as a target volume and the contralateral breast, ipsilateral lung, contralateral lung and heart tissues as organs at risk (OAR). IMRT with seven beams (IMRT7), nine beams (IMRT9) and 11 beams (IMRT11) plans were developed and compared with CTT and among each other. The conformity index (CI), homogeneity index (HI), and doses to OAR were compared to each other.
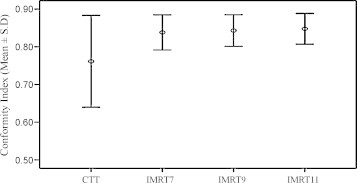
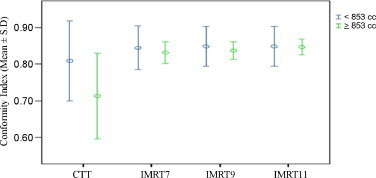
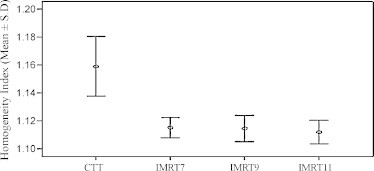
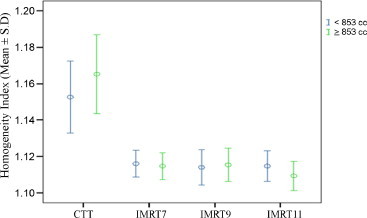
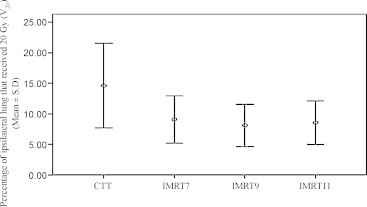
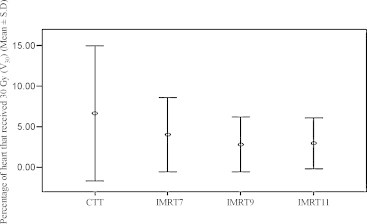
Results: ALL OF IMRT PLANS SIGNIFICANTLY IMPROVED CI (CTT: 0.76; IMRT7: 0.84; IMRT9: 0.84; IMRT11: 0.85), HI (CTT: 1.16; IMRT7: 1.12; IMRT9: 1.11; IMRT11: 1.11), volume of the ipsilateral lung receiving more than 20 Gy (>V20 Gy) (CTT: 14.6; IMRT7: 9.08; IMRT9: 8.10; IMRT11: 8.60), and volume of the heart receiving more than 30 Gy (>V30 Gy) (CTT: 6.7; IMRT7: 4.04; IMRT9: 2.80; IMRT11: 2.98) compared to CTT. All IMRT plans were found to significantly decrease >V20 Gy and >V30 Gy volumes compared to conformal plans. But IMRT plans increased the volume of OAR receiving low dose radiotherapy: volume of contralateral lung receiving 5 and 10 Gy (CTT: 0.0-0.0; IMRT7: 19.0-0.7; IMRT9: 17.2-0.66; IMRT11: 18.7-0.58, respectively) and volume of contralateral breast receiving 10 Gy (CTT: 0.03; IMRT7: 0.38; IMRT9: 0.60; IMRT11: 0.68). The differences among IMRT plans with increased number of beams were not statistically significant.
Conclusion: IMRT significantly improved conformity and homogeneity index for plans. Heart and lung volumes receiving high doses were decreased, but OAR receiving low doses was increased.
Keywords: Breast cancer; Conventional techniques comparison; IMRT; Left breast; Whole breast radiotherapy.
Figures
References
-
- Beckham W., Popescu C.C., Patenaude V.V. Is multibeam IMRT better than standard treatment for patients with left-sided breast cancer? Int J Radiat Oncol Biol Phys. 2007;69:918–924. - PubMed
-
- Rongsriyam K., Rojpornpradit P., Lertbutsayanukul C. Dosimetric study of inverse-planned intensity modulated, forward-planned intensity modulated and conventional tangential techniques in breast conserving radiotherapy. J Med Assoc Thai. 2008;91:1571–1582. - PubMed
-
- Popescu C.C., Olivotto I., Patenaude V.V. Inverse-planned, dynamic, multi-beam, intensity-modulated radiation therapy (IMRT): a promising technique when target volume is the left breast and internal mammary lymph nodes. Med Dosim. 2006;31:283–291. - PubMed
-
- Oliver M., Chen J., Wong E. A treatment planning study comparing whole breast radiation therapy against conformal, IMRT and tomotherapy for accelerated partial breast irradiation. Radiother Oncol. 2007;82:317–323. - PubMed
-
- Mayo C.S., Urie M.M., Fitzgerald T.J. Hybrid IMRT plans-concurrently treating conventional and IMRT beams for improved breast irradiation and reduced planning time. Int J Radiat Oncol Biol Phys. 2005;61:922–932. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
