

Lymph node staging in colorectal cancer: old controversies and recent advances
- PMID: 24379568
- PMCID: PMC3870496
- DOI: 10.3748/wjg.v19.i46.8515
Lymph node staging in colorectal cancer: old controversies and recent advances
Abstract
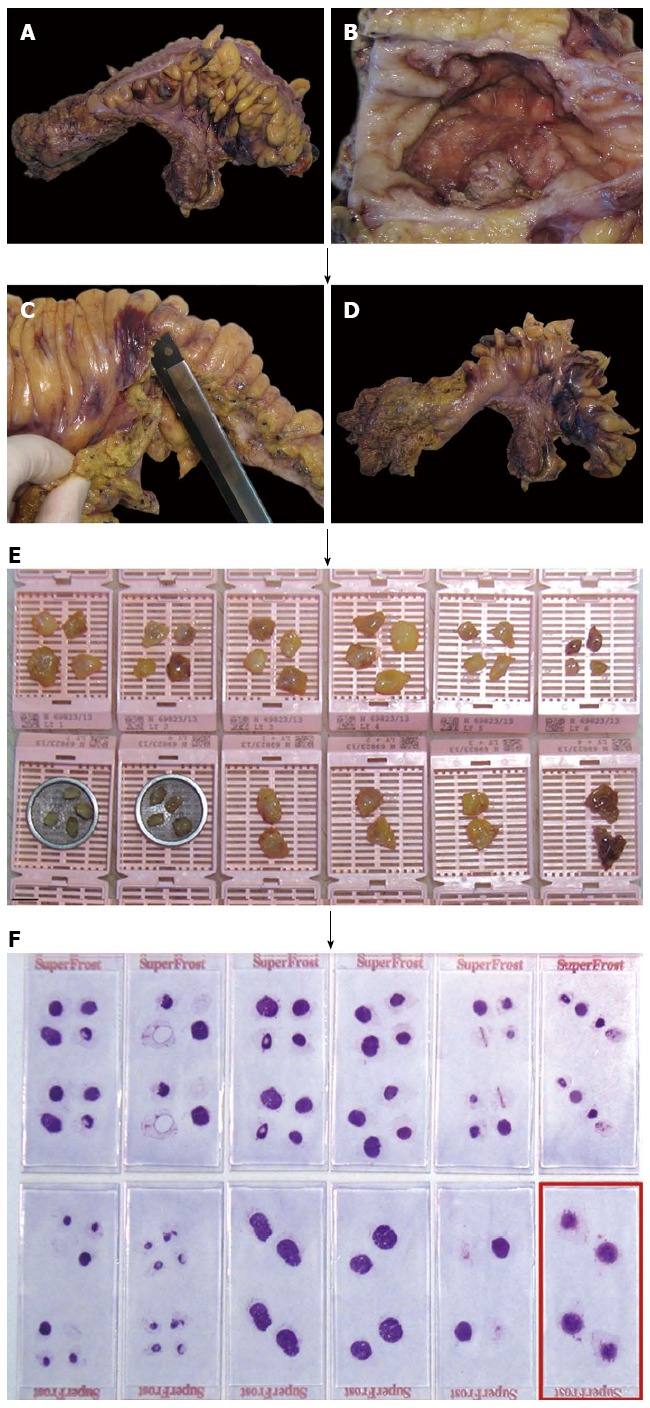
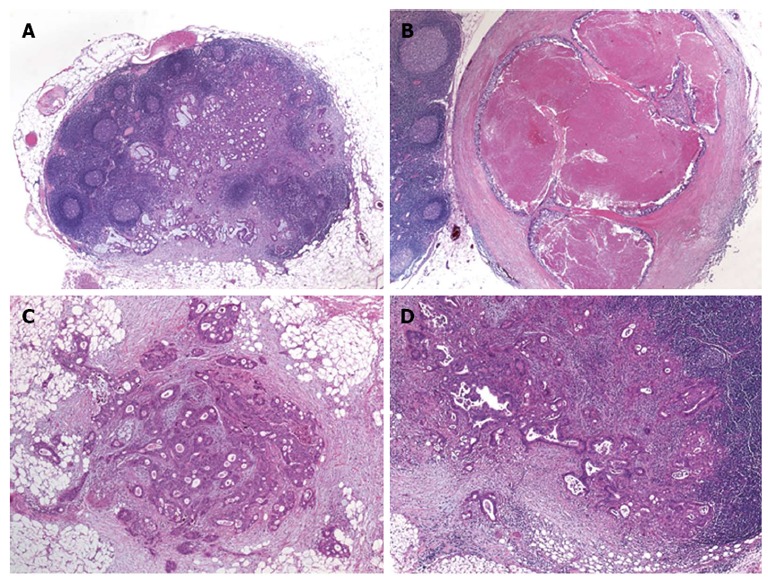
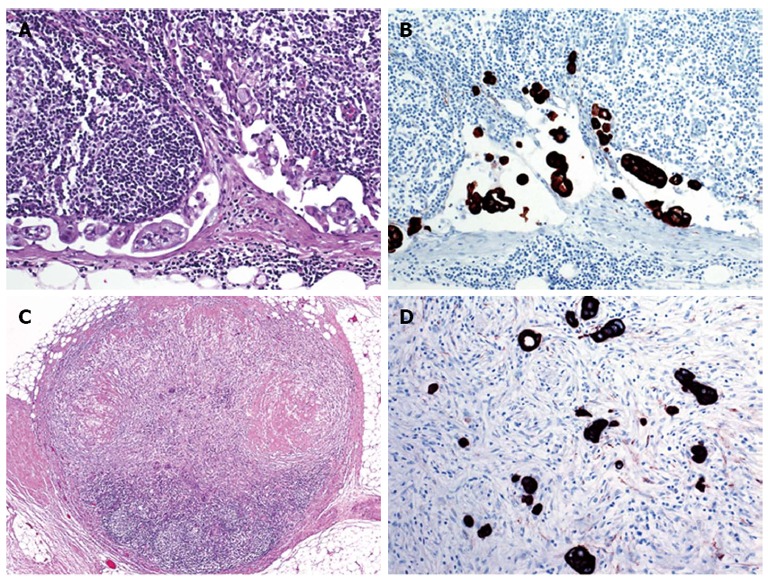
Outcome prediction based on tumor stage reflected by the American Joint Committee on Cancer (AJCC)/Union for International Cancer Control (UICC) tumor node metastasis (TNM) system is currently regarded as the strongest prognostic parameter for patients with colorectal cancer. For affected patients, the indication for adjuvant therapy is mainly guided by the presence of regional lymph node metastasis. In addition to the extent of surgical lymph node removal and the thoroughness of the pathologist in dissecting the resection specimen, several parameters that are related to the pathological work-up of the dissected nodes may affect the clinical significance of lymph node staging. These include changing definitions of lymph nodes, involved lymph nodes, and tumor deposits in different editions of the AJCC/UICC TNM system as well as the minimum number of nodes to be dissected. Methods to increase the lymph node yield in the fatty tissue include methylene blue injection and acetone compression. Outcome prediction based on the lymph node ratio, defined as the number of positive lymph nodes divided by the total number of retrieved nodes, may be superior to the absolute numbers of involved nodes. Extracapsular invasion has been identified as additional prognostic factor. Adding step sectioning and immunohistochemistry to the pathological work-up may result in higher accuracy of histological diagnosis. The clinical value of more recent technical advances, such as sentinel lymph node biopsy and molecular analysis of lymph nodes tissue still remains to be defined.
Keywords: Colon cancer; Extracapsular invasion; Immunohistochemistry; Lymph node metastasis; Lymph node ratio; Molecular analysis; Prognosis; Rectum cancer; Sentinel lymph node; Tumor staging.
Figures
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63:11–30. - PubMed
-
- Washington MK. Colorectal carcinoma: selected issues in pathologic examination and staging and determination of prognostic factors. Arch Pathol Lab Med. 2008;132:1600–1607. - PubMed
-
- Benson AB, Arnoletti JP, Bekaii-Saab T, Chan E, Chen YJ, Choti MA, Cooper HS, Dilawari RA, Engstrom PF, Enzinger PC, et al. Colon cancer. J Natl Compr Canc Netw. 2011;9:1238–1290. - PubMed
-
- Benson AB, Bekaii-Saab T, Chan E, Chen YJ, Choti MA, Cooper HS, Engstrom PF, Enzinger PC, Fakih MG, Fuchs CS, et al. Rectal cancer. J Natl Compr Canc Netw. 2012;10:1528–1564. - PubMed
-
- Nagtegaal ID, Tot T, Jayne DG, McShane P, Nihlberg A, Marshall HC, Påhlman L, Brown JM, Guillou PJ, Quirke P. Lymph nodes, tumor deposits, and TNM: are we getting better? J Clin Oncol. 2011;29:2487–2492. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
