

Localized type 1 autoimmune pancreatitis superimposed upon preexisting intraductal papillary mucinous neoplasms
- PMID: 24379640
- PMCID: PMC3870568
- DOI: 10.3748/wjg.v19.i47.9127
Localized type 1 autoimmune pancreatitis superimposed upon preexisting intraductal papillary mucinous neoplasms
Abstract
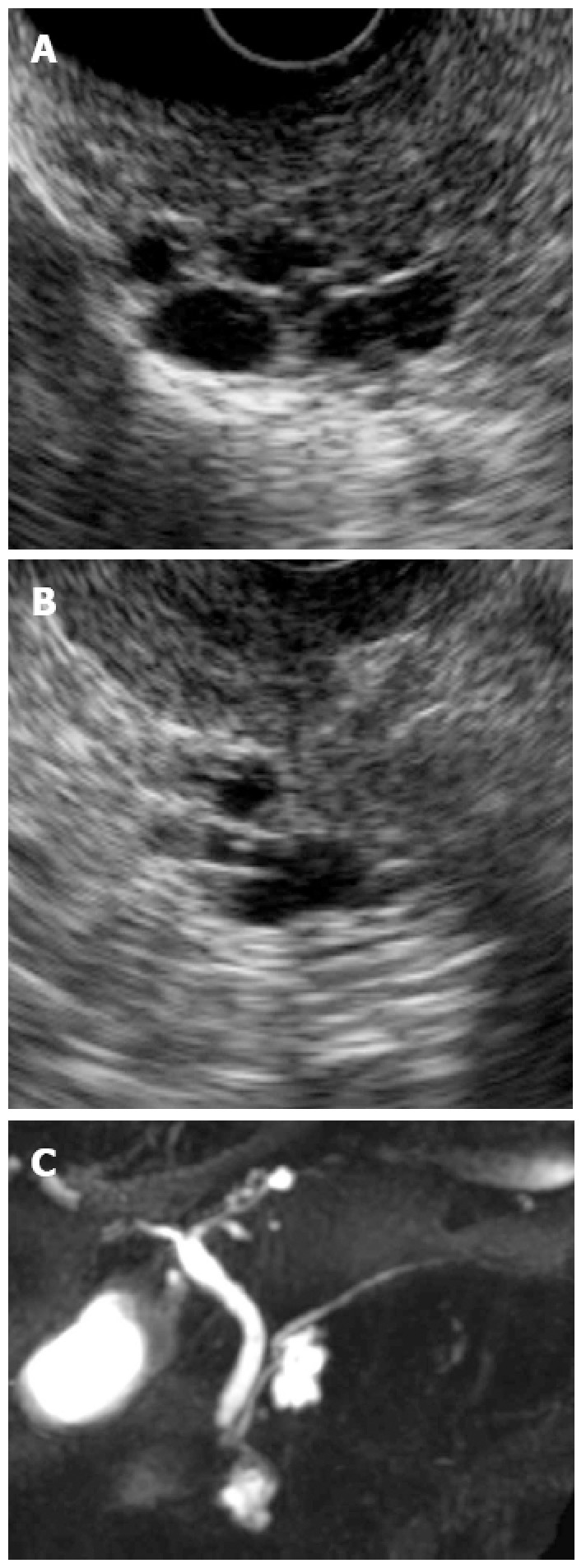
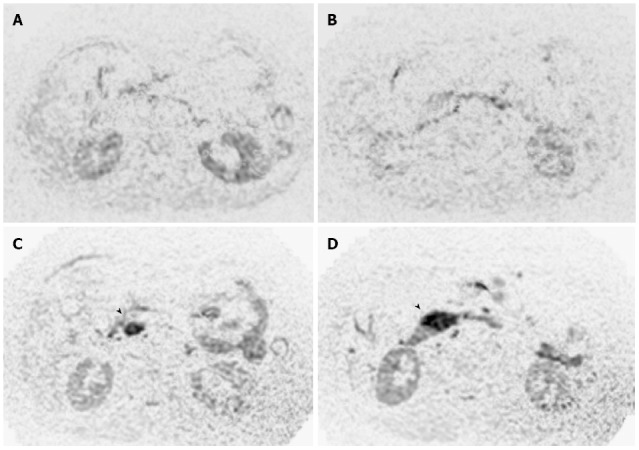
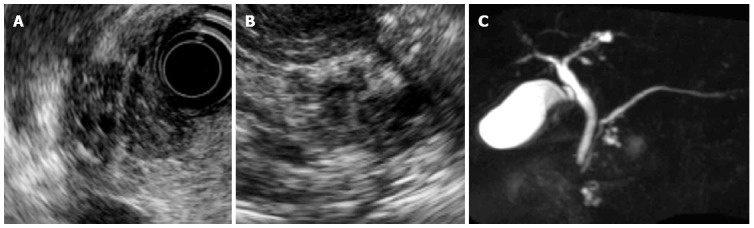
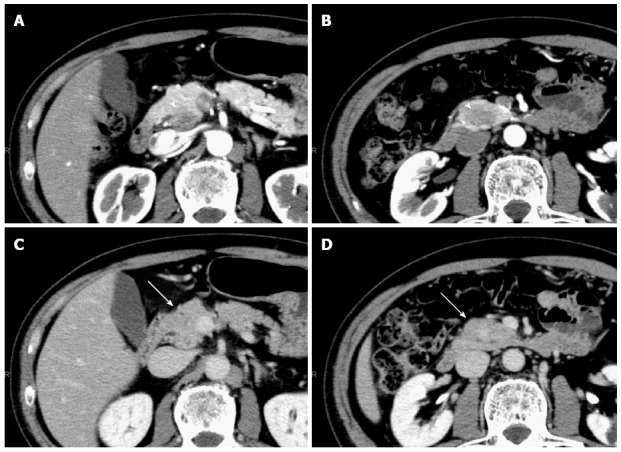
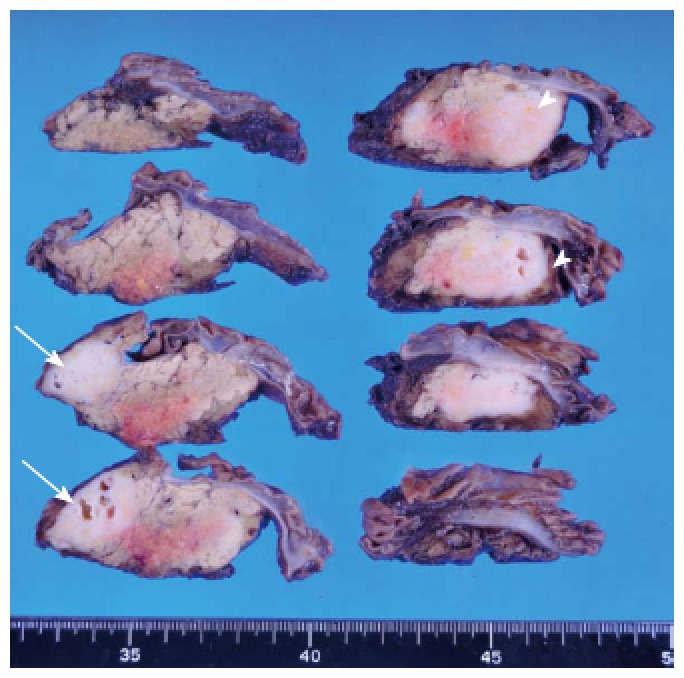
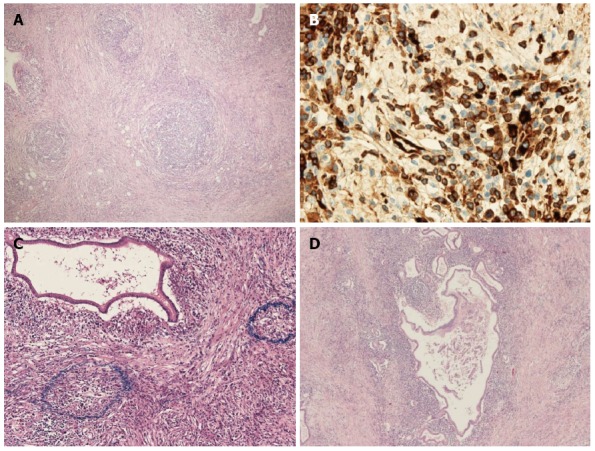
A 70-year-old woman was found to have 2 cystic lesions in the head of the pancreas on abdominal ultrasonography during a routine medical examination. Endoscopic ultrasonography (EUS) and magnetic resonance cholangiopancreatography showed multilocular cysts in the head of the pancreas without dilation of the main pancreatic duct. The patient was followed-up semiannually with imaging studies for suspected branch duct-type intraductal papillary mucinous neoplasm (IPMN). At 3 years after initial presentation, hypoechoic lesions were observed around each pancreatic cyst by EUS. Diffusion-weighted imaging showed high-intensity regions corresponding to these lesions. Therefore, a diagnosis of invasive carcinoma derived from IPMN could not be excluded, and subtotal stomach-preserving pancreaticoduodenectomy was performed. The macroscopic examination of the surgical specimen showed whitish solid masses in the head of the pancreas, with multilocular cysts within each mass. Microscopically, each solid mass consisted of inflammatory cells such as lymphocytes and plasma cells. Furthermore, immunochemical staining revealed immunoglobulin G4-positive cells, and many obliterating phlebitides were observed. The cysts consisted of mucus-producing epithelial cells and showed a papillary growth pattern. Based on these findings, we diagnosed multiple localized type 1 autoimmune pancreatitis occurring only in the vicinity of the branch duct-type IPMN.
Keywords: Autoimmune pancreatitis; Diffusion-weighted imaging; Endoscopic ultrasonography; Immunoglobulin G4; Intraductal papillary mucinous neoplasm.
Figures
References
-
- Shimosegawa T, Chari ST, Frulloni L, Kamisawa T, Kawa S, Mino-Kenudson M, Kim MH, Klöppel G, Lerch MM, Löhr M, et al. International consensus diagnostic criteria for autoimmune pancreatitis: guidelines of the International Association of Pancreatology. Pancreas. 2011;40:352–358. - PubMed
-
- Buscarini E, Frulloni L, De Lisi S, Falconi M, Testoni PA, Zambelli A. Autoimmune pancreatitis: a challenging diagnostic puzzle for clinicians. Dig Liver Dis. 2010;42:92–98. - PubMed
-
- Catalano MF, Sahai A, Levy M, Romagnuolo J, Wiersema M, Brugge W, Freeman M, Yamao K, Canto M, Hernandez LV. EUS-based criteria for the diagnosis of chronic pancreatitis: the Rosemont classification. Gastrointest Endosc. 2009;69:1251–1261. - PubMed
-
- Gardner TB, Levy MJ, Takahashi N, Smyrk TC, Chari ST. Misdiagnosis of autoimmune pancreatitis: a caution to clinicians. Am J Gastroenterol. 2009;104:1620–1623. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
