

Short-term vs. long-term heart rate variability in ischemic cardiomyopathy risk stratification
- PMID: 24379785
- PMCID: PMC3862074
- DOI: 10.3389/fphys.2013.00364
Short-term vs. long-term heart rate variability in ischemic cardiomyopathy risk stratification
Abstract
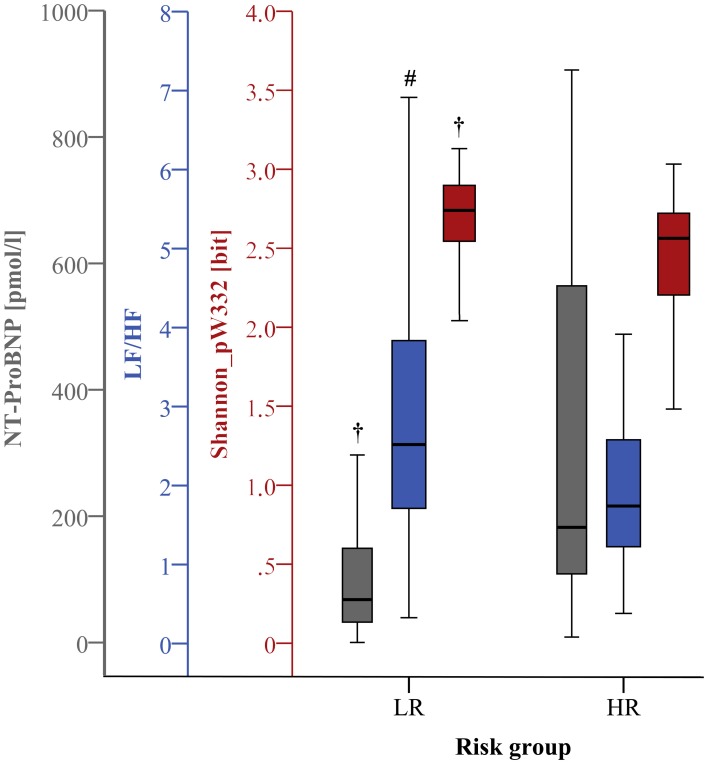
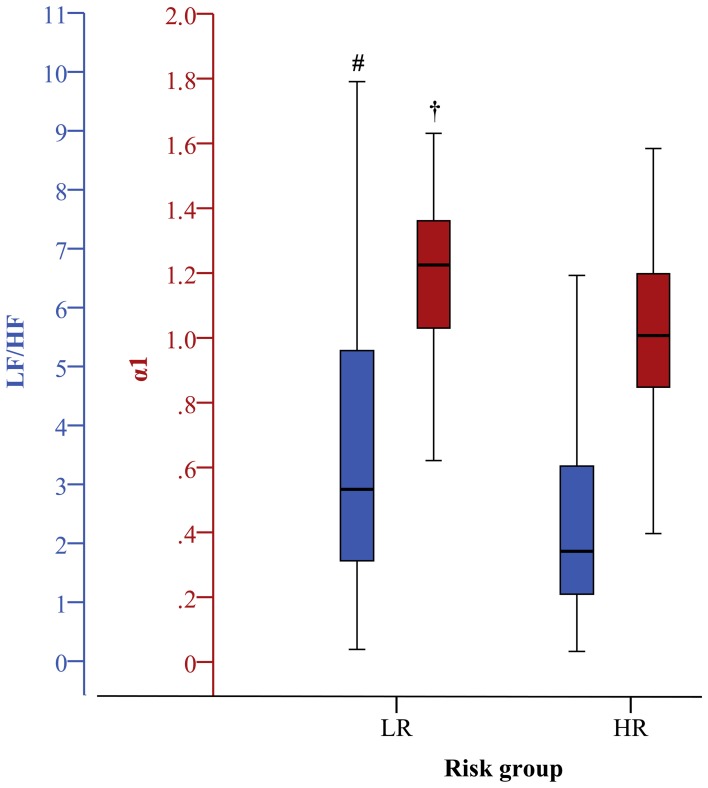
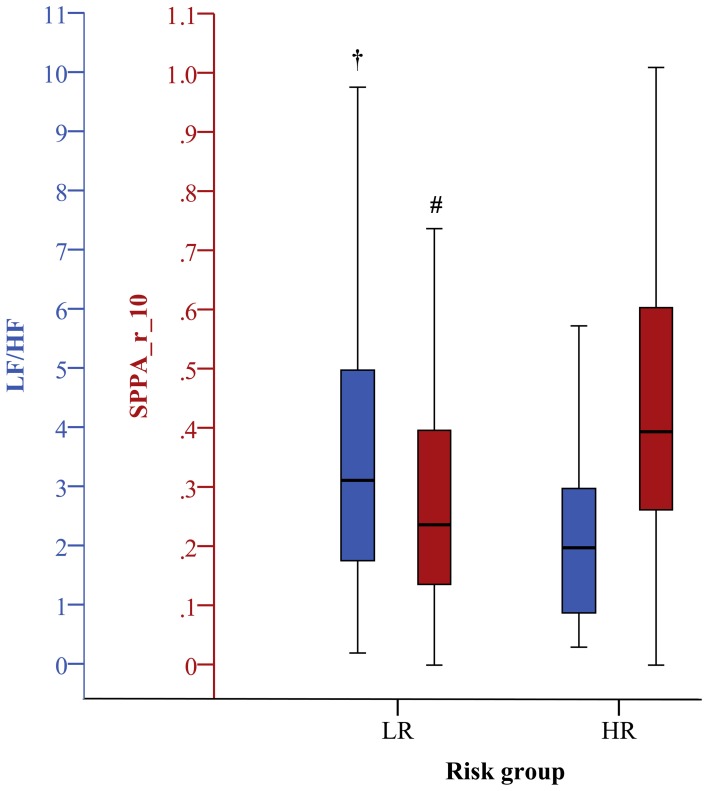
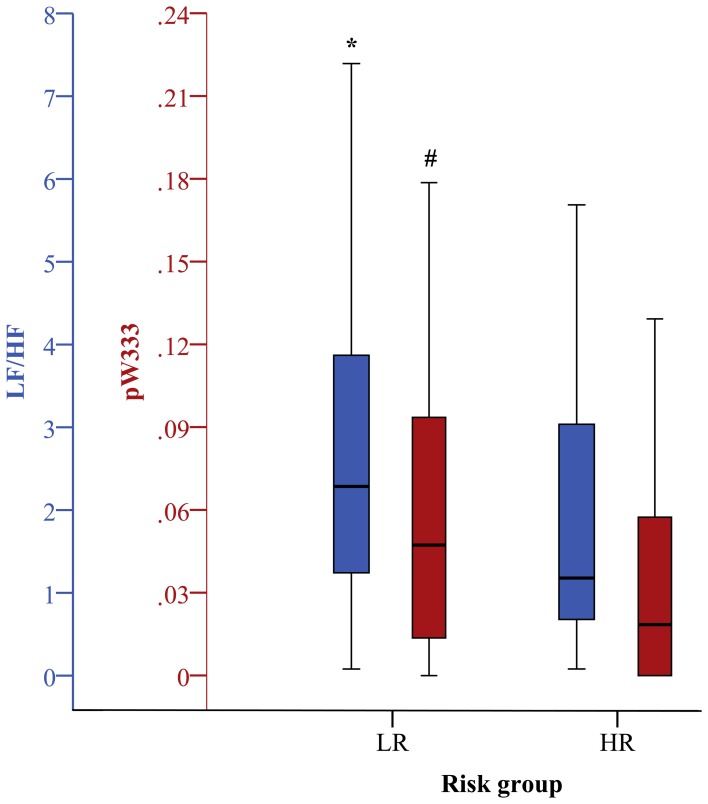
In industrialized countries with aging populations, heart failure affects 0.3-2% of the general population. The investigation of 24 h-ECG recordings revealed the potential of nonlinear indices of heart rate variability (HRV) for enhanced risk stratification in patients with ischemic heart failure (IHF). However, long-term analyses are time-consuming, expensive, and delay the initial diagnosis. The objective of this study was to investigate whether 30 min short-term HRV analysis is sufficient for comparable risk stratification in IHF in comparison to 24 h-HRV analysis. From 256 IHF patients [221 at low risk (IHFLR) and 35 at high risk (IHFHR)] (a) 24 h beat-to-beat time series (b) the first 30 min segment (c) the 30 min most stationary day segment and (d) the 30 min most stationary night segment were investigated. We calculated linear (time and frequency domain) and nonlinear HRV analysis indices. Optimal parameter sets for risk stratification in IHF were determined for 24 h and for each 30 min segment by applying discriminant analysis on significant clinical and non-clinical indices. Long- and short-term HRV indices from frequency domain and particularly from nonlinear dynamics revealed high univariate significances (p < 0.01) discriminating between IHFLR and IHFHR. For multivariate risk stratification, optimal mixed parameter sets consisting of 5 indices (clinical and nonlinear) achieved 80.4% AUC (area under the curve of receiver operating characteristics) from 24 h HRV analysis, 84.3% AUC from first 30 min, 82.2 % AUC from daytime 30 min and 81.7% AUC from nighttime 30 min. The optimal parameter set obtained from the first 30 min showed nearly the same classification power when compared to the optimal 24 h-parameter set. As results from stationary daytime and nighttime, 30 min segments indicate that short-term analyses of 30 min may provide at least a comparable risk stratification power in IHF in comparison to a 24 h analysis period.
Keywords: daytime; heart rate variability; ischemic cardiomyopathy; long-term; nighttime; nonlinear dynamics; risk stratification; short-term.
Figures
Similar articles
-
Enhanced detection of abnormalities in heart rate variability and dynamics by 7-day continuous ECG monitoring.Ann Noninvasive Electrocardiol. 2022 Jan;27(1):e12897. doi: 10.1111/anec.12897. Epub 2021 Sep 21. Ann Noninvasive Electrocardiol. 2022. PMID: 34546637 Free PMC article.
-
Ischemic risk stratification by means of multivariate analysis of the heart rate variability.Physiol Meas. 2013 Mar;34(3):325-38. doi: 10.1088/0967-3334/34/3/325. Epub 2013 Feb 12. Physiol Meas. 2013. PMID: 23399982
-
Automatic sleep staging using empirical mode decomposition, discrete wavelet transform, time-domain, and nonlinear dynamics features of heart rate variability signals.Comput Methods Programs Biomed. 2013 Oct;112(1):47-57. doi: 10.1016/j.cmpb.2013.06.007. Epub 2013 Jul 26. Comput Methods Programs Biomed. 2013. PMID: 23895941
-
The prognostic value of heart rate variability in the elderly, changing the perspective: from sympathovagal balance to chaos theory.Pacing Clin Electrophysiol. 2012 May;35(5):622-38. doi: 10.1111/j.1540-8159.2012.03335.x. Epub 2012 Feb 21. Pacing Clin Electrophysiol. 2012. PMID: 22352300 Review.
-
An Overview of Heart Rate Variability Metrics and Norms.Front Public Health. 2017 Sep 28;5:258. doi: 10.3389/fpubh.2017.00258. eCollection 2017. Front Public Health. 2017. PMID: 29034226 Free PMC article. Review.
Cited by
-
Prediction of major adverse cardiovascular events in patients with acute coronary syndrome: Development and validation of a non-invasive nomogram model based on autonomic nervous system assessment.Front Cardiovasc Med. 2022 Nov 3;9:1053470. doi: 10.3389/fcvm.2022.1053470. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36407419 Free PMC article.
-
Slow 0.1 Hz Breathing and Body Posture Induced Perturbations of RRI and Respiratory Signal Complexity and Cardiorespiratory Coupling.Front Physiol. 2020 Feb 14;11:24. doi: 10.3389/fphys.2020.00024. eCollection 2020. Front Physiol. 2020. PMID: 32132926 Free PMC article.
-
Validity of the Polar V800 monitor for measuring heart rate variability in mountain running route conditions.Eur J Appl Physiol. 2018 Mar;118(3):669-677. doi: 10.1007/s00421-018-3808-0. Epub 2018 Jan 22. Eur J Appl Physiol. 2018. PMID: 29356949
-
Implications of heart rate variability measured using wearable electrocardiogram devices in diagnosing Parkinson's disease and its association with neuroimaging biomarkers: a case-control study.Front Aging Neurosci. 2025 May 12;17:1530240. doi: 10.3389/fnagi.2025.1530240. eCollection 2025. Front Aging Neurosci. 2025. PMID: 40421102 Free PMC article.
-
Increased prevalence of cardiac autonomic dysfunction at different degrees of glucose intolerance in the general population: the KORA S4 survey.Diabetologia. 2015 May;58(5):1118-28. doi: 10.1007/s00125-015-3534-7. Epub 2015 Feb 28. Diabetologia. 2015. PMID: 25724570
References
-
- Bilchick K. C., Fetics B., Djoukeng R., Fisher S. G., Fletcher R. D., Singh S. N., et al. (2002). Prognostic value of heart rate variability in chronic congestive heart failure (Veterans Affairs' Survival Trial of Antiarrhythmic Therapy in Congestive Heart Failure). Am. J. Cardiol. 90, 24–28 10.1016/S0002-9149(02)02380-9 - DOI - PubMed
-
- Bleumink G. S., Knetsch A. M., Sturkenboom M. C., Straus S. M., Hofman A., Deckers J. W., et al. (2004). Quantifying the heart failure epidemic: prevalence, incidence rate, lifetime risk and prognosis of heart failure. The Rotterdam Study. Eur. Heart J. 25, 1614–1619 10.1016/j.ehj.2004.06.038 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials