

Biological effects of green tea capsule supplementation in pre-surgery postmenopausal breast cancer patients
- PMID: 24380073
- PMCID: PMC3861892
- DOI: 10.3389/fonc.2013.00298
Biological effects of green tea capsule supplementation in pre-surgery postmenopausal breast cancer patients
Abstract
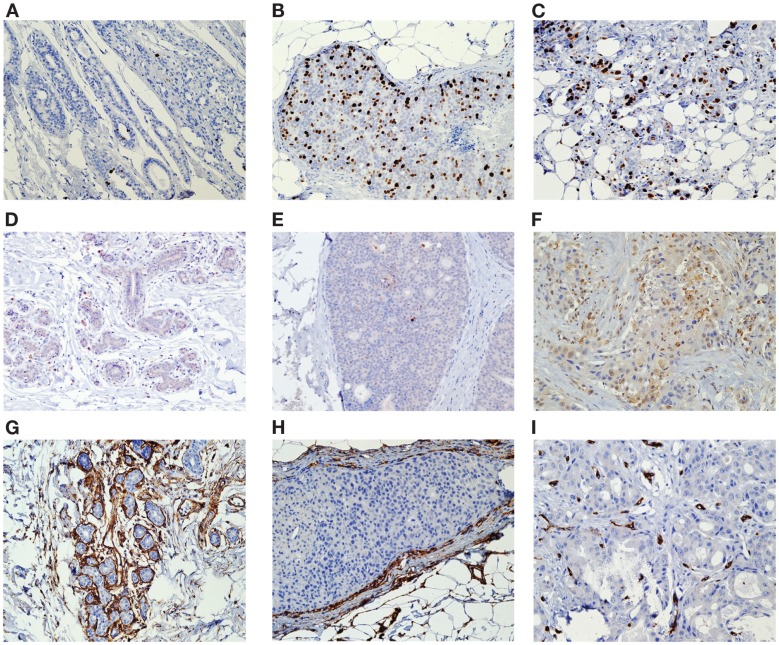
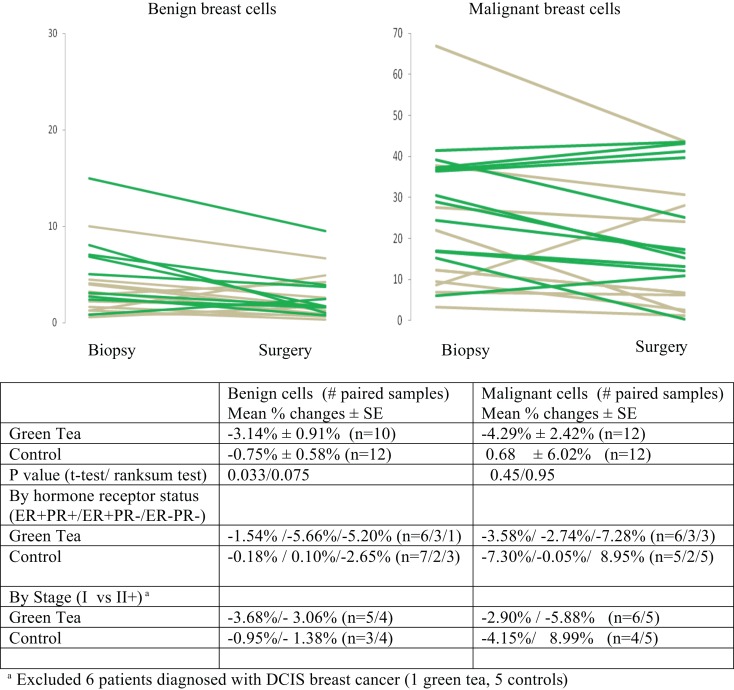
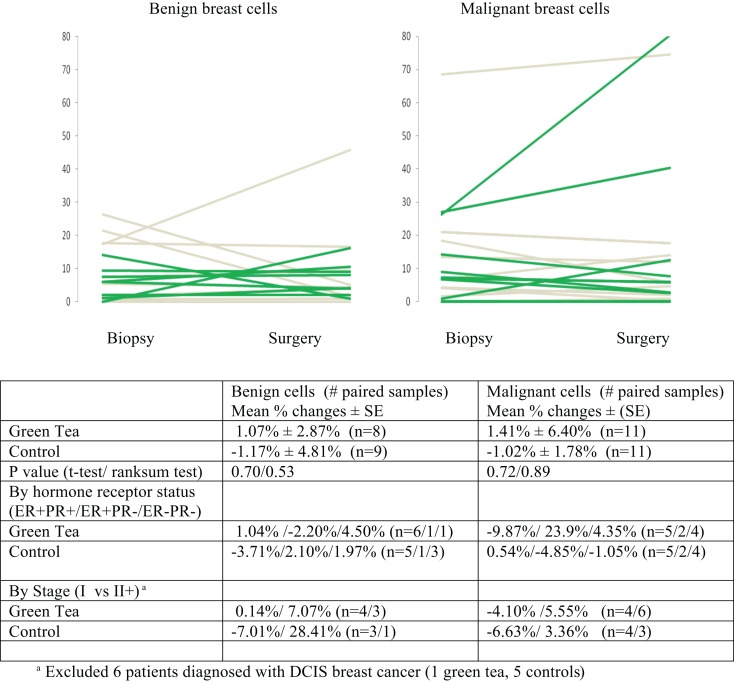
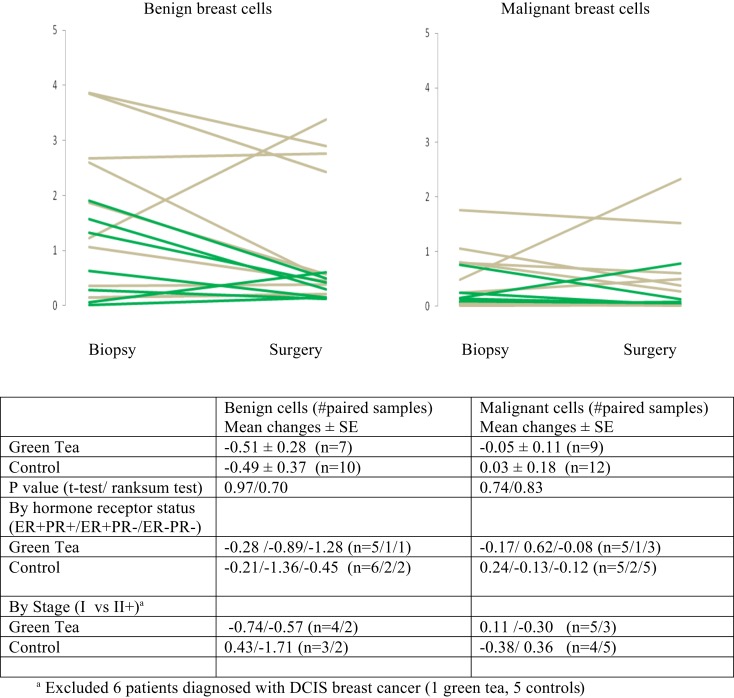
Regular green tea intake has been associated with an inverse risk of breast cancer. There are compelling experimental evidence that green tea, particularly, epigallocatechin gallate, the most potent green tea catechin, possesses a range of anti-cancer properties. We conducted a pre-surgical study of green tea capsules vs. no-green tea in women with primary breast cancer to determine the effects of green tea supplementation on markers of biological response. Postmenopausal women with ductal carcinoma in situ (DCIS) or stage I or II breast cancer took green tea capsules (940 mg per day) for an average of 35 days prior to surgery (n = 13) or received no green tea (n = 18). Paired diagnostic core biopsy and surgical specimen samples were analyzed for cell proliferation (Ki-67), apoptosis (caspase-3), and angiogenesis (CD34) separately in benign and malignant cell components. There were no significant changes in caspase-3 and CD34 in the green tea and no green tea groups and there were no significant differences in the change in these markers between the two groups. However, Ki-67 levels declined in both benign and malignant cell components in the green tea group; the decline in Ki-67 positivity in malignant cells was not statistically significant (P = 0.10) but was statistically significant in benign cells (P = 0.007). Ki-67 levels in benign and malignant cells did not change significantly in the no green tea group. There was a statistically significant difference in the change in Ki-67 in benign cells (P = 0.033) between the green tea and the no green tea groups. The trend of a consistent reduction in Ki-67 in both benign and malignant cells in the green tea group warrants further investigations in a larger study of breast cancer patients or high-risk women.
Keywords: chemoprevention; green tea; postmenopausal breast cancer.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials