

Metabolic syndrome prevalence and associations in a bariatric surgery cohort from the Longitudinal Assessment of Bariatric Surgery-2 study
- PMID: 24380645
- PMCID: PMC3942706
- DOI: 10.1089/met.2013.0116
Metabolic syndrome prevalence and associations in a bariatric surgery cohort from the Longitudinal Assessment of Bariatric Surgery-2 study
Abstract
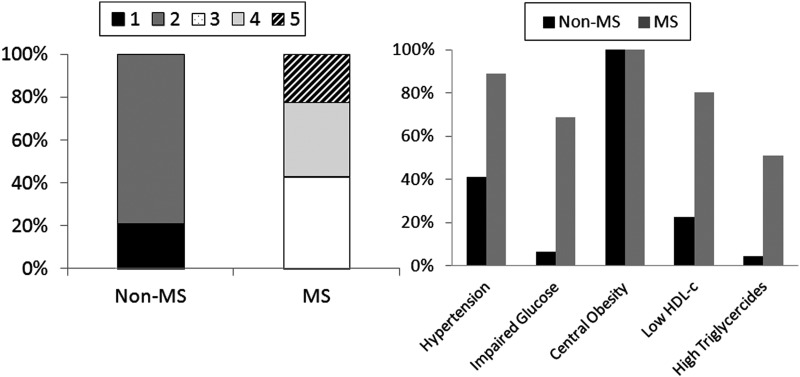
Background: Metabolic syndrome is associated with higher risk for cardiovascular disease, sleep apnea, and nonalcoholic steatohepatitis, all common conditions in patients referred for bariatric surgery, and it may predict early postoperative complications. The objective of this study was to determine the prevalence of metabolic syndrome, defined using updated National Cholesterol Education Program criteria, in adults undergoing bariatric surgery and compare the prevalence of baseline co-morbid conditions and select operative and 30-day postoperative outcomes by metabolic syndrome status.
Methods: Complete metabolic syndrome data were available for 2275 of 2458 participants enrolled in the Longitudinal Assessment of Bariatric Surgery-2 (LABS-2), an observational cohort study designed to evaluate long-term safety and efficacy of bariatric surgery in obese adults.
Results: The prevalence of metabolic syndrome was 79.9%. Compared to those without metabolic syndrome, those with metabolic syndrome were significantly more likely to be men, to have a higher prevalence of diabetes and prior cardiac events, to have enlarged livers and higher median levels of liver enzymes, a history of sleep apnea, and a longer length of stay after surgery following laparoscopic Roux-en-Y gastric bypass (RYGB) and gastric sleeves but not open RYGB or laparoscopic adjustable gastric banding. Metabolic syndrome status was not significantly related to duration of surgery or rates of composite end points of intraoperative events and 30-day major adverse surgical outcomes.
Conclusions: Nearly four in five participants undergoing bariatric surgery presented with metabolic syndrome. Establishing a diagnosis of metabolic syndrome in bariatric surgery patients may identify a high-risk patient profile, but does not in itself confer a higher risk for short-term adverse postsurgery outcomes.
Figures
References
-
- Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001;285:2486–2497 - PubMed
-
- Alberti KG, Eckel RH, Grundy SM, et al. . Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009;120:1640–1645 - PubMed
-
- Mottillo S, Filion KB, Genest J, et al. . The metabolic syndrome and cardiovascular risk a systematic review and meta-analysis. J Am Coll Cardiol 2010;56:1113–1132 - PubMed
-
- Wilson PW, D'Agostino RB, Parise H, et al. . Metabolic syndrome as a precursor of cardiovascular disease and type 2 diabetes mellitus. Circulation 2005;112:3066–3072 - PubMed
-
- Buchwald H, Avidor Y, Braunwald E, et al. . Bariatric surgery: A systematic review and meta-analysis. JAMA 2004;292:1724–1737 - PubMed
Publication types
MeSH terms
Grants and funding
- UL1 TR000005/TR/NCATS NIH HHS/United States
- UL1-RR024153/RR/NCRR NIH HHS/United States
- U01-DK66526/DK/NIDDK NIH HHS/United States
- M01RR-00037/RR/NCRR NIH HHS/United States
- UL1TR000128/TR/NCATS NIH HHS/United States
- U01-DK66667/DK/NIDDK NIH HHS/United States
- UL1-RR024996/RR/NCRR NIH HHS/United States
- U01-DK66555/DK/NIDDK NIH HHS/United States
- U01-DK66568/DK/NIDDK NIH HHS/United States
- DCC-U01 DK066557/DK/NIDDK NIH HHS/United States
- UL1 TR000457/TR/NCATS NIH HHS/United States
- U01-DK66471/DK/NIDDK NIH HHS/United States
- U01-DK66585/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials