

Comparison of pre-bent titanium mesh versus polyethylene implants in patient specific orbital reconstructions
- PMID: 24382118
- PMCID: PMC4029398
- DOI: 10.1186/1746-160X-9-32
Comparison of pre-bent titanium mesh versus polyethylene implants in patient specific orbital reconstructions
Abstract
Introduction: Computerized tomography DICOM file can be relatively easily transformed to a virtual 3D model. With the help of additional software we are able to create the mirrored model of an undamaged orbit and on this basis produce an individual implant for the patient Authors decided to apply implants with any thickness, which are authors own invention to obtain volumetric support and more stable orbital wall reconstruction outcome. Material of choice was ultra-high molecular weight polyethylene (UHMWPE).
Objective: The aim of this study was to present and compare functional results of individual reconstructions of orbital wall using either titanium mesh or ultra-high molecular weight polyethylene.
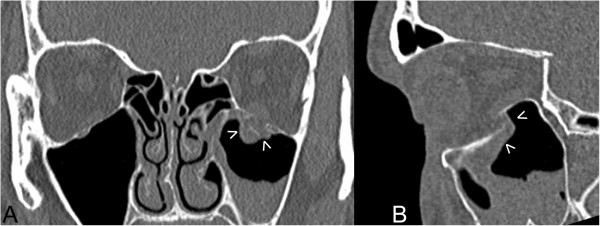
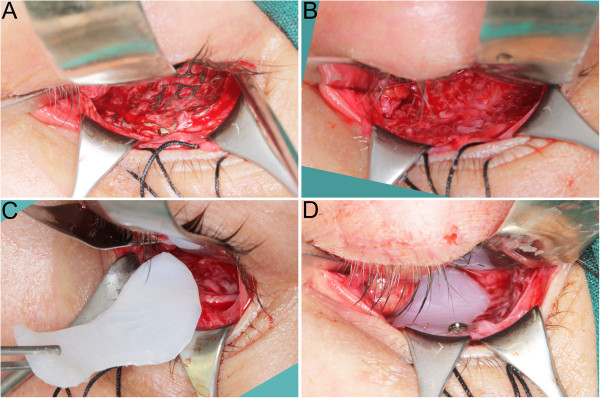
Materials and methods: 57 consecutive patients affected by orbital wall fracture (46 males, 11 females, mean age 34±14 year) were treated in Department of Maxillofacial Surgery from 2010 to 2012. In the first group we used patient specific treatment by titanium mesh shaped on a 3D printed model of a mirrored intact orbit (37 orbits) or by individually manufactured UHMW-PE implantby CAM milling in second group (20 orbits). All of these patients were subjected to preoperative helical computerized tomography and consultation of an ophthalmologist (including binocular single vision loss test - BSVL). Further on, patients were operated under general anaesthesia using transconjuctival approach. BSVL was again evaluated post-operationally in 1 month and 6 months later.
Results: Functional treatment results (BSVL) for both groups were similar in 1 month as well as 6 months post operational time. There was no statistically significant difference between these two groups.
Conclusions: This study of 6 months functional result assessment of pre-bent individual implants and CNC milled ultra-high molecular weight polyethylene of the orbital wall has shown it to be a predictable reconstruction method. Individually shaped UHMWPE seems to be as good as pre-bent titanium mesh.
Figures




Similar articles
-
Technical concept of patient-specific, ultrahigh molecular weight polyethylene orbital wall implant.J Craniomaxillofac Surg. 2013 Jun;41(4):282-90. doi: 10.1016/j.jcms.2012.10.007. Epub 2013 Jan 18. J Craniomaxillofac Surg. 2013. PMID: 23333489
-
Classical versus custom orbital wall reconstruction: Selected factors regarding surgery and hospitalization.J Craniomaxillofac Surg. 2017 May;45(5):710-715. doi: 10.1016/j.jcms.2017.02.008. Epub 2017 Feb 17. J Craniomaxillofac Surg. 2017. PMID: 28318927
-
Computer-aided orbital wall defects treatment by individual design ultrahigh molecular weight polyethylene implants.J Craniomaxillofac Surg. 2014 Jun;42(4):283-9. doi: 10.1016/j.jcms.2013.05.015. Epub 2013 Jul 5. J Craniomaxillofac Surg. 2014. PMID: 23835569
-
Orbital surgery: state of the art.Oral Maxillofac Surg Clin North Am. 2010 Feb;22(1):59-71. doi: 10.1016/j.coms.2009.11.006. Oral Maxillofac Surg Clin North Am. 2010. PMID: 20159478 Review.
-
[Advances in the research and application of orbital blowout fracture repair material].Zhonghua Yan Ke Za Zhi. 2019 Nov 11;55(11):876-880. doi: 10.3760/cma.j.issn.0412-4081.2019.11.019. Zhonghua Yan Ke Za Zhi. 2019. PMID: 31715684 Review. Chinese.
Cited by
-
Controversies and Contemporary Management of Orbital Floor Fractures.Craniomaxillofac Trauma Reconstr. 2022 Sep;15(3):237-245. doi: 10.1177/19433875211026430. Epub 2021 Jun 24. Craniomaxillofac Trauma Reconstr. 2022. PMID: 36081678 Free PMC article. Review.
-
Plastic Surgery Innovation with 3D Printing for Craniomaxillofacial Operations.Mo Med. 2020 Mar-Apr;117(2):136-142. Mo Med. 2020. PMID: 32308239 Free PMC article.
-
A systematic review of implant materials for facial reconstructive and aesthetic surgery.Front Surg. 2025 Mar 28;12:1548597. doi: 10.3389/fsurg.2025.1548597. eCollection 2025. Front Surg. 2025. PMID: 40225117 Free PMC article.
-
3D-printing techniques in a medical setting: a systematic literature review.Biomed Eng Online. 2016 Oct 21;15(1):115. doi: 10.1186/s12938-016-0236-4. Biomed Eng Online. 2016. PMID: 27769304 Free PMC article.
-
New and emerging patient-centered CT imaging and image-guided treatment paradigms for maxillofacial trauma.Emerg Radiol. 2018 Oct;25(5):533-545. doi: 10.1007/s10140-018-1616-9. Epub 2018 Jun 20. Emerg Radiol. 2018. PMID: 29922866 Review.
References
-
- Roden KS, Tong W, Surrusco M, Shockley WW, Van Aalst JA, Hultman CS. Changing characteristics of facial fractures treated at a regional, level 1 trauma center, from 2005 to 2010: an assessment of patient demographics, referral patterns, etiology of injury, anatomic location, and clinical outcomes. Ann Plas Surg. 2012;9:461–466. doi: 10.1097/SAP.0b013e31823b69dd. - DOI - PubMed
-
- Loba P, Kozakiewicz M, Nowakowska O, Omulecki W, Broniarczyk-Loba A. Management of persistent diplopia after surgical repair of orbital fractures. J AAPOS: the official publication of the American Association for Pediatric Ophthalmology and Strabismus / American Association for Pediatric Ophthalmology and Strabismus. 2012;9:548–553. doi: 10.1016/j.jaapos.2012.08.007. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
