

Interleukin 6 and apolipoprotein E as predictors of acute brain dysfunction and survival in critical care patients
- PMID: 24382617
- PMCID: PMC4809634
- DOI: 10.4037/ajcc2014578
Interleukin 6 and apolipoprotein E as predictors of acute brain dysfunction and survival in critical care patients
Abstract
Background: Delirium occurs in up to 80% of intensive care patients and is associated with poor outcomes. The biological cause of delirium remains elusive.
Objectives: To determine if delirium and recovery are associated with serum levels of interleukins and apolipoprotein E over time and with apolipoprotein E genotype.
Methods: The sample consisted of 77 patients with no previous cognitive deficits who required mechanical ventilation for 24 to 96 hours. Daily serum samples were obtained for enzyme-linked immunosorbent assay measurements of interleukins 6, 8, and 10 and apolipoprotein E. DNA extracted from blood was analyzed for apolipoprotein E genotyping. The Confusion Assessment Method for the Intensive Care Unit was administered daily on days 2 through 9.
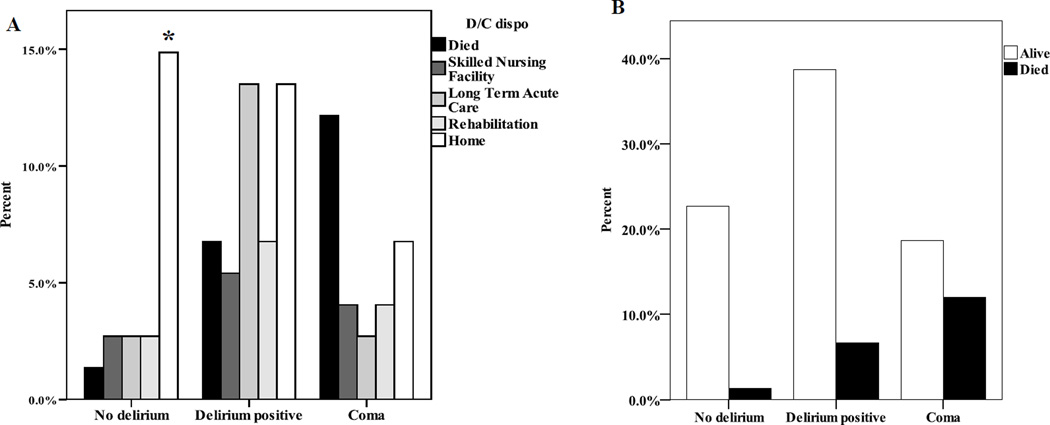
Results: Among the 77 patients, 23% had no delirium, 46% experienced delirium, and 31% experienced coma. Additionally, 77% had delirium or coma (acute brain dysfunction), and compared with other patients, had fewer ventilator-free days (P = .03), longer stay (P = .04), higher care needs at discharge (P = .001), higher mortality (P = .02), and higher levels of interleukin 6 (P = .03), and the APOE*3/*3 apolipoprotein E genotype (P = .05). Serum levels of apolipoprotein E correlated with levels of interleukins 8 and 10. Patients with the E4 allele of apolipoprotein E had shorter duration of delirium (P = .02) and lower mortality (P = .03) than did patients without this allele.
Conclusions: Apolipoprotein E plays a complex role in illness response and recovery in critically ill patients. The relationship between apolipoprotein E genotype and brain dysfunction and survival is unclear.
Figures


Comment in
-
Evidence-based review and discussion points.Am J Crit Care. 2014 Jan;23(1):58-9. doi: 10.4037/ajcc2014113. Am J Crit Care. 2014. PMID: 24516931 No abstract available.
Similar articles
-
Evidence-based review and discussion points.Am J Crit Care. 2014 Jan;23(1):58-9. doi: 10.4037/ajcc2014113. Am J Crit Care. 2014. PMID: 24516931 No abstract available.
-
Apolipoprotein E4 polymorphism as a genetic predisposition to delirium in critically ill patients.Crit Care Med. 2007 Jan;35(1):112-7. doi: 10.1097/01.CCM.0000251925.18961.CA. Crit Care Med. 2007. PMID: 17133176
-
Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit.JAMA. 2004 Apr 14;291(14):1753-62. doi: 10.1001/jama.291.14.1753. JAMA. 2004. PMID: 15082703
-
APOE and cytokines as biological markers for recovery of prevalent delirium in elderly medical inpatients.Int J Geriatr Psychiatry. 2007 Jul;22(7):688-94. doi: 10.1002/gps.1732. Int J Geriatr Psychiatry. 2007. PMID: 17203511
-
Evaluating early administration of the hydroxymethylglutaryl-CoA reductase inhibitor simvastatin in the prevention and treatment of delirium in critically ill ventilated patients (MoDUS trial): study protocol for a randomized controlled trial.Trials. 2015 May 16;16:218. doi: 10.1186/s13063-015-0731-0. Trials. 2015. PMID: 25982544 Free PMC article. Clinical Trial.
Cited by
-
Serum biomarkers of delirium in critical illness: a systematic review of mechanistic and diagnostic evidence.Intensive Care Med Exp. 2025 Sep 1;13(1):90. doi: 10.1186/s40635-025-00795-z. Intensive Care Med Exp. 2025. PMID: 40889075 Free PMC article. Review.
-
Antipsychotic Use for ICU Delirium and Associated Inflammatory Markers.J Intensive Care Med. 2024 Apr;39(4):313-319. doi: 10.1177/08850666231201567. Epub 2023 Sep 19. J Intensive Care Med. 2024. PMID: 37724016 Free PMC article.
-
The American Geriatrics Society/National Institute on Aging Bedside-to-Bench Conference: Research Agenda on Delirium in Older Adults.J Am Geriatr Soc. 2015 May;63(5):843-52. doi: 10.1111/jgs.13406. Epub 2015 Mar 31. J Am Geriatr Soc. 2015. PMID: 25834932 Free PMC article.
-
Development and validation of risk-stratification delirium prediction model for critically ill patients: A prospective, observational, single-center study.Medicine (Baltimore). 2017 Jul;96(29):e7543. doi: 10.1097/MD.0000000000007543. Medicine (Baltimore). 2017. PMID: 28723773 Free PMC article.
-
Common Data Elements for Disorders of Consciousness: Recommendations from the Working Group on Biospecimens and Biomarkers.Neurocrit Care. 2024 Feb;40(1):58-64. doi: 10.1007/s12028-023-01883-2. Epub 2023 Dec 12. Neurocrit Care. 2024. PMID: 38087173
References
-
- Ouimet S, Kavanagh BP, Gottfried SB, Skrobik T. Incidence, risk factors and consequences of ICU delirium. Intensive Care Med. 2007;33(1):66–73. - PubMed
-
- van Eijk MMJ, Slooter AJC. Delirium in intensive care unit patients. Semin Cardiothorac Vasc Anesth. 2010;14(2):141–147. - PubMed
-
- Witlox J, Eurelings LSM, de Jonghe JFM, Kalisvaart KJ, Eikelenboom P, van Gool WA. Delirium in elderly patients and the risk of postdischarge mortality, institutionalization, and dementia: a meta-analysis. JAMA. 2010;304(4):443–451. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
