

Tempering pediatric hospitalist supervision of residents improves admission process efficiency without decreasing quality of care
- PMID: 24382752
- PMCID: PMC4103017
- DOI: 10.1002/jhm.2138
Tempering pediatric hospitalist supervision of residents improves admission process efficiency without decreasing quality of care
Abstract
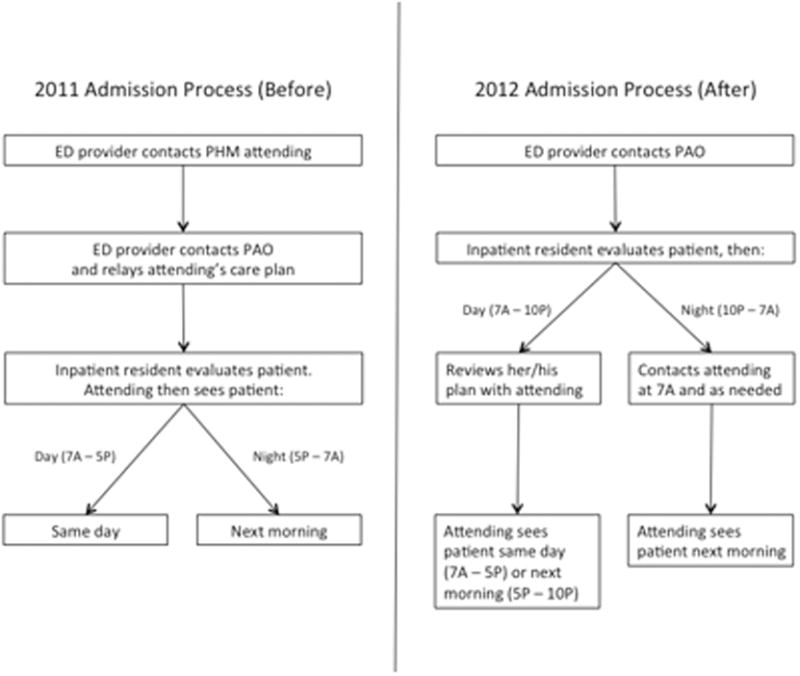
Background: Many academic pediatric hospital medicine (PHM) divisions have recently increased in-house supervision of residents, often providing 24/7 in-house attending coverage. Contrary to this trend, we removed mandated PHM attending input during the admission process. We present an evaluation of this process change.
Methods: This cohort study compared outcomes between patients admitted to the PHM service before (July 1, 2011-September 30, 2011) and after (July 1, 2012-September 30, 2012) the process change. We evaluated time from admission request to inpatient orders, length of stay (LOS), frequency of change in antibiotic choice, and rapid response team (RRT) calls within 24 hours of admission. Data were obtained via chart abstraction and from administrative databases. Wilcoxon rank sum and Fisher exact tests were used for analysis.
Results: We identified 182 and 210 admissions in the before and after cohorts, respectively. Median time between emergency department admission request and inpatient orders was significantly shorter after the change (123 vs 62 minutes, P < 0.001). We found no significant difference in LOS, the number of changes to initial resident antibiotic choice, standard of care, or RRTs called within the first 24 hours of admission.
Conclusion: Removing mandated attending input in decision making for PHM admissions significantly decreased time to inpatient resident admission orders without a change in measurable clinical outcomes.
© 2013 Society of Hospital Medicine.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Accreditation Council for Graduate Medical Education Task Force on Quality Care and Professionalism. The ACGME 2011 duty hour standards: enhancing quality of care, supervision, and resident professional development. Accreditation Council for Graduate Medical Education; Chicago, Ill: 2011.
-
- Moonesinghe SR, Lowery J, Shahi N, Millen A, Beard JD. Impact of reduction in working hours for doctors in training on postgraduate medical education and patients' outcomes: systemic review. BMJ. 2011;342:d1580. - PubMed
-
- Feig BA, Hasso AN. ACGME 2011 duty-hour guidelines: consequences expected by radiology residency directors and chief residents. J Am Coll Radiol. 2012;9(11):820–7. - PubMed
-
- Chiong W. Justifying patient risks associated with medical education. JAMA. 2007;298(9):1046–8. - PubMed
-
- Gosdin C, Simmons J, Yau C, Sucharew H, Carlson D, Paciorkowski N. Survey of academic pediatric pospitalist programs in the U.S.: organizational, administrative and financial factors. J Hosp Med. 2013;8(6):285–91. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
