

National trends in utilization and outcomes of coronary revascularization procedures among people with and without type 2 diabetes in Spain (2001-2011)
- PMID: 24383412
- PMCID: PMC3881504
- DOI: 10.1186/1475-2840-13-3
National trends in utilization and outcomes of coronary revascularization procedures among people with and without type 2 diabetes in Spain (2001-2011)
Abstract
Background: Diabetes is associated with a high risk of death due to coronary artery disease (CAD). People with diabetes suffering from CAD are frequently treated with revascularization procedures. We aim to compare trends in the use and outcomes of coronary revascularization procedures in diabetic and non-diabetic patients in Spain between 2001 and 2011.
Methods: We identified all patients who had undergone coronary revascularization procedures, percutaneous coronary interventions (PCI) and coronary artery bypass graft (CABG) surgeries, using national hospital discharge data. Discharges were grouped by diabetes status: type 2 diabetes and no diabetes. The incidence of discharges attributed to coronary revascularization procedures were calculated stratified by diabetes status. We calculated length of stay and in-hospital mortality (IHM). We apply joinpoint log-linear regression to identify the years in which changes in tendency occurred in the use of PCI and CABG in diabetic and non-diabetic patients. Multivariate analysis was adjusted by age, sex, year and comorbidity (Charlson comorbidity index).
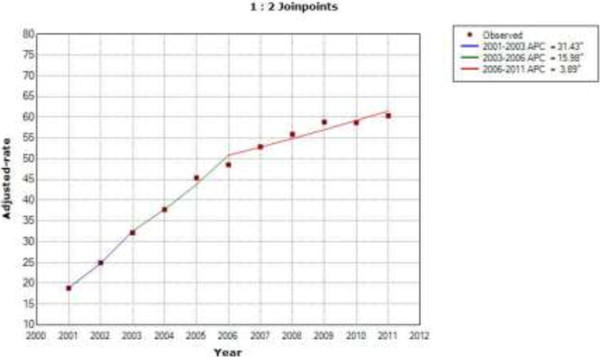
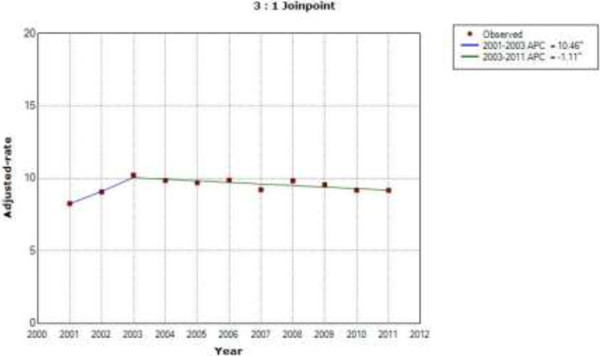
Results: From 2001 to 2011, 434,108 PCIs and 79,986 CABGs were performed. According to the results of the joinpoint analysis, we found that sex and age-adjusted use of PCI increased by 31.4% per year from 2001 to 2003, by 15.9% per year from 2003 to 2006 and by 3.8% per year from 2006 to 2011 in patients with diabetes. IHM among patients with diabetes who underwent a PCI did not change significantly over the entire study period (OR 0.99; 95% CI 0.97-1.00).Among patients with diabetes who underwent a CABG, the sex and age-adjusted CABG incidence rate increased by 10.4% per year from 2001 to 2003, and then decreased by 1.1% through 2011. Diabetic patients who underwent a CABG had a 0.67 (95% CI 0.63-0.71) times lower probability of dying during hospitalization than those without diabetes.
Conclusions: The annual percent change in PCI procedures increased in diabetic and non-diabetic patients. Higher comorbidity and the female gender are associated with a higher IHM in PCI procedures. In diabetic and non-diabetic patients, we found a decrease in the use of CABG procedures. IHM was higher in patients without diabetes than in those with diabetes.
Figures
References
-
- Nelson SE. Management of patients with type 2 diabetes. Endocrinol Nutr. 2002;49:113–126. doi: 10.1016/S1575-0922(02)74441-0. - DOI
-
- Norhammar A, Lindback J, Ryden L, Wallentin L, Stenestrand U. Improved but still high short- and long-term mortality rates after myocardial infarction in patients with diabetes mellitus: A time-trend report from the Swedish Register of Information and Knowledge about Swedish Heart Intensive Care Admission. Heart. 2007;93:1577–1583. - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
