

Prevalence trends in respiratory symptoms and asthma in relation to smoking - two cross-sectional studies ten years apart among adults in northern Sweden
- PMID: 24383710
- PMCID: PMC3929247
- DOI: 10.1186/1939-4551-7-1
Prevalence trends in respiratory symptoms and asthma in relation to smoking - two cross-sectional studies ten years apart among adults in northern Sweden
Abstract
Background: Smoking is considered to be the single most important preventable risk factor for respiratory symptoms. Estimating prevalence of respiratory symptoms is important since they most often precede a diagnosis of an obstructive airway disease, which places a major burden on the society. The aim of this study was to estimate prevalence trends of respiratory symptoms and asthma among Swedish adults, in relation to smoking habits. A further aim was to estimate the proportion of respiratory symptom and asthma prevalence attributable to smoking.
Methods: Data from two large-scale cross-sectional surveys among adults performed in northern Sweden in 1996 and 2006 were analysed. Identical methods and the same questionnaire were used in both surveys. The association between smoking, respiratory symptoms and asthma was analysed with multiple logistic regression analyses. Changes in prevalence of respiratory symptoms and asthma from 1996 to 2006 were expressed as odds ratios. Additionally, the population attributable risks of smoking were estimated.
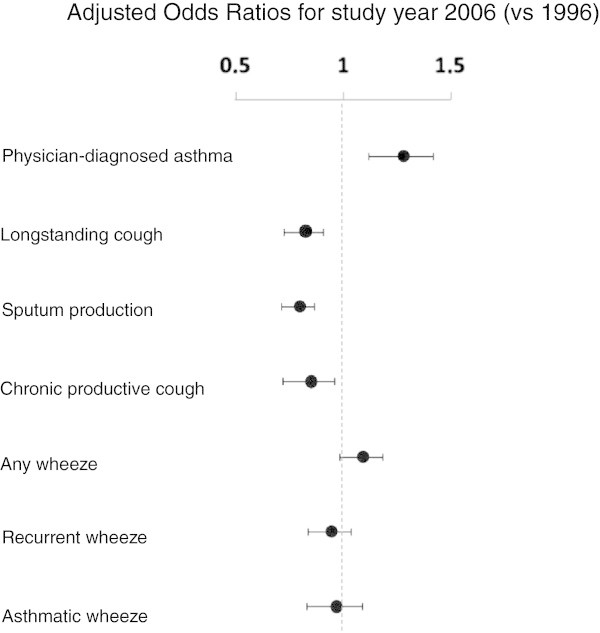
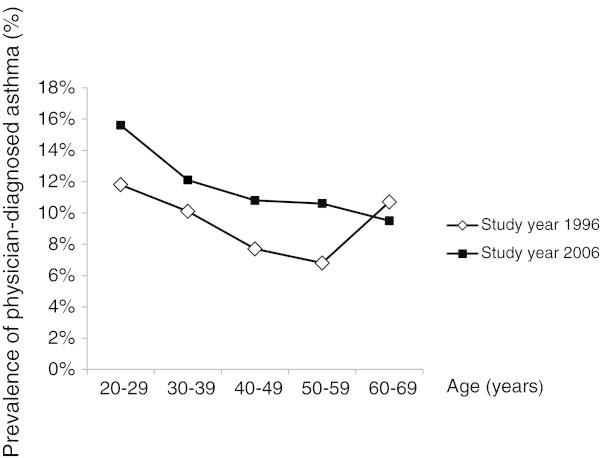
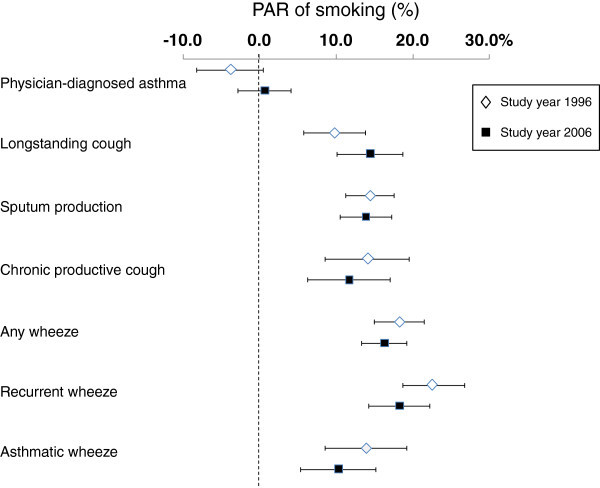
Results: The prevalence of most respiratory symptoms decreased significantly from 1996 to 2006. Longstanding cough decreased from 12.4 to 10.1%, sputum production from 19.0 to 15.0%, chronic productive cough from 7.3 to 6.2%, and recurrent wheeze from 13.4 to 12.0%. Any wheeze and asthmatic wheeze remained unchanged. This parallels to a decrease in smoking from 27.4 to 19.1%. In contrast, physician-diagnosed asthma increased from 9.4 to 11.6%. The patterns were similar after correction for confounders. All respiratory symptoms were highly associated with smoking, and the proportion of respiratory symptoms in the population attributed to smoking (PAR) ranged from 9.8 to 25.5%. In 2006, PAR of smoking was highest for recurrent wheeze (20.6%).
Conclusions: In conclusion, we found that respiratory symptoms, in particular symptoms common in bronchitis, decreased among adults in northern Sweden, parallel to a decrease in smoking from 1996 to 2006. In contrast, the prevalence of physician-diagnosed asthma increased during the same time-period. Up to one fourth of the respiratory symptom prevalence in the population was attributable to smoking.
Figures
References
-
- Eriksen M, Mackay J, Ross H. The Tobacco Atlas by the World Lung Foundation & American Cancer Society. Available at: http://www.tobaccoatlas.org. Accessed 04/03, 2013.
-
- Jarvis A. A study on liability and the health costs of smoking. DG SANCO (2008/C6/046) UPDATED FINAL REPORT April 2012. 2013. Available at: http://ec.europa.eu/health/tobacco/products/revision/index_en.htm. Accessed 27/12, 2013.
-
- Slama K. Global perspective on tobacco control. Part I. The global state of the tobacco epidemic. Int J Tuberc Lung Dis. 2008;7(1):3–7. - PubMed
-
- Bjerg A, Ekerljung L, Middelveld R, Dahlen SE, Forsberg B, Franklin K. et al. Increased prevalence of symptoms of rhinitis but not of asthma between 1990 and 2008 in Swedish adults: comparisons of the ECRHS and GA(2)LEN surveys. PLoS One. 2011;7(2):e16082. doi: 10.1371/journal.pone.0016082. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
