

Risk factors for the development of parastomal hernia after radical cystectomy
- PMID: 24384155
- PMCID: PMC4156556
- DOI: 10.1016/j.juro.2013.12.041
Risk factors for the development of parastomal hernia after radical cystectomy
Abstract
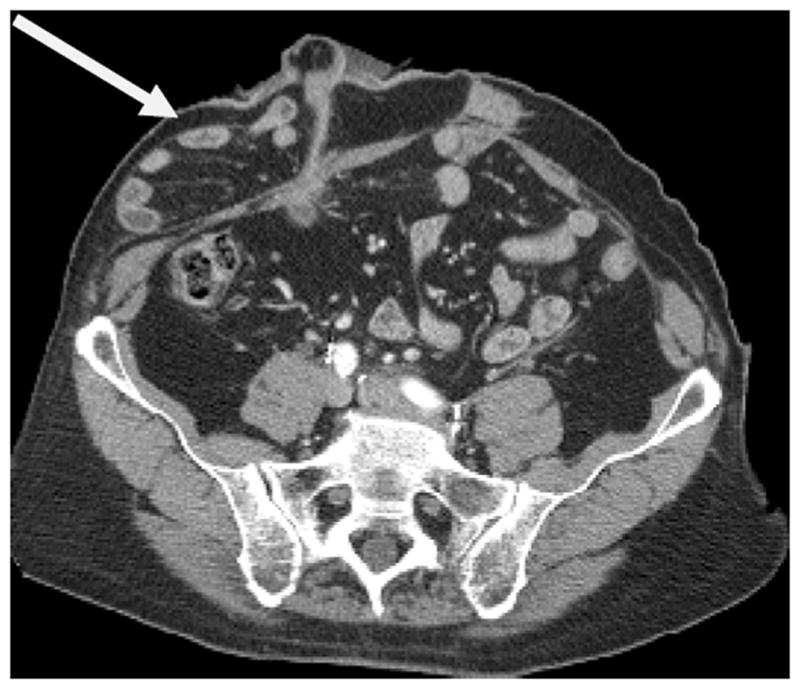
Purpose: Parastomal hernia is a frequent complication of stoma formation after radical cystectomy. We determined the prevalence and risk factors for the development of parastomal hernia after radical cystectomy.
Materials and methods: We conducted a retrospective study of 433 consecutive patients who underwent open radical cystectomy and ileal conduit between 2006 and 2010. Postoperative cross-sectional imaging studies performed for routine oncologic followup (1,736) were evaluated for parastomal hernia, defined as radiographic evidence of protrusion of abdominal contents through the abdominal wall defect created by forming the stoma. Univariable and multivariable Cox regression analyses were used to determine clinical and surgical factors associated with parastomal hernia.
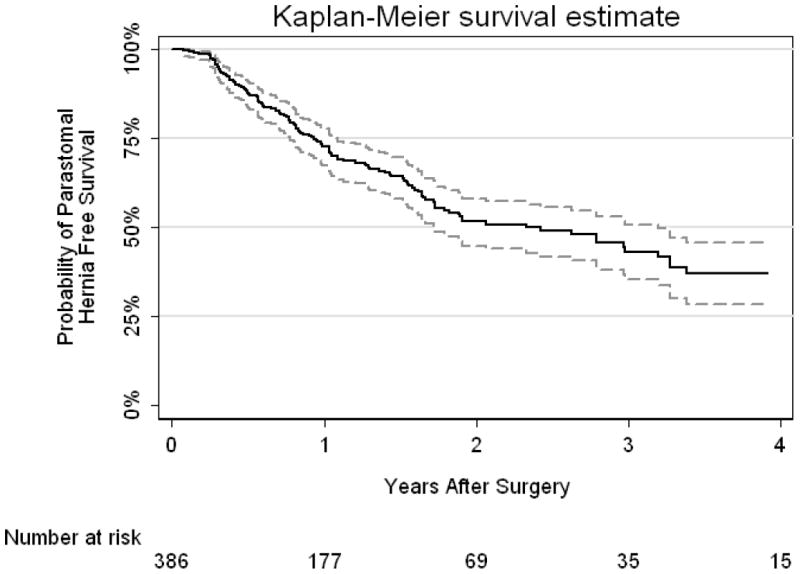
Results: Complete data were available for 386 patients with radiographic parastomal hernia occurring in 136. The risk of a parastomal hernia developing was 27% (95% CI 22, 33) and 48% (95% CI 42, 55) at 1 and 2 years, respectively. Clinical diagnosis of parastomal hernia was documented in 93 patients and 37 were symptomatic. Of 16 patients with clinical parastomal hernia referred for repair 8 had surgery. On multivariable analysis female gender (HR 2.25; 95% CI 1.58, 3.21; p<0.0001), higher body mass index (HR 1.08 per unit increase; 95% CI 1.05, 1.12; p<0.0001) and lower preoperative albumin (HR 0.43 per gm/dl; 95% CI 0.25, 0.75; p=0.003) were significantly associated with parastomal hernia.
Conclusions: The overall risk of radiographic evidence of parastomal hernia approached 50% at 2 years. Female gender, higher body mass index and lower preoperative albumin were most associated with the development of parastomal hernia. Identifying those at greatest risk may allow for prospective surgical maneuvers at the time of initial surgery, such as placement of prophylactic mesh in selected patients, to prevent the occurrence of parastomal hernia.
Keywords: cystectomy; hernia; risk factors.
Copyright © 2014 American Urological Association Education and Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures


References
-
- Farnham SB, Cookson MS. Surgical complications of urinary diversion. World J Urol. 2004;22:157. - PubMed
-
- Kouba E, Sands M, Lentz A, et al. Incidence and risk factors of stomal complications in patients undergoing cystectomy with ileal conduit urinary diversion for bladder cancer. J Urol. 2007;178:950. - PubMed
-
- Pearl RK. Parastomal hernias. World J Surg. 1989;13:569. - PubMed
-
- Israelsson LA. Parastomal hernias. Surg Clin North Am. 2008;88:113. - PubMed
-
- Goligher JC, Lloyd-Davies OV, Robertson CT. Small-gut obstructions following combined excision of the rectum with special reference to strangulation round the colostomy. Br J Surg. 1951;38:467. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
