

Glycaemic control improves perfusion recovery and VEGFR2 protein expression in diabetic mice following experimental PAD
- PMID: 24385342
- PMCID: PMC3928005
- DOI: 10.1093/cvr/cvt342
Glycaemic control improves perfusion recovery and VEGFR2 protein expression in diabetic mice following experimental PAD
Abstract
Aims: Diabetes mellitus (DM) is associated with poor clinical outcomes in humans with peripheral arterial disease (PAD) and in pre-clinical models of PAD, but the effects of glycaemic control are poorly understood. We investigated the effect of glycaemic control on experimental PAD in mice with Type 1 DM and explored the effects of hyperglycaemia on vascular endothelial growth factor receptor 2 (VEGFR2) expression in ischaemia.
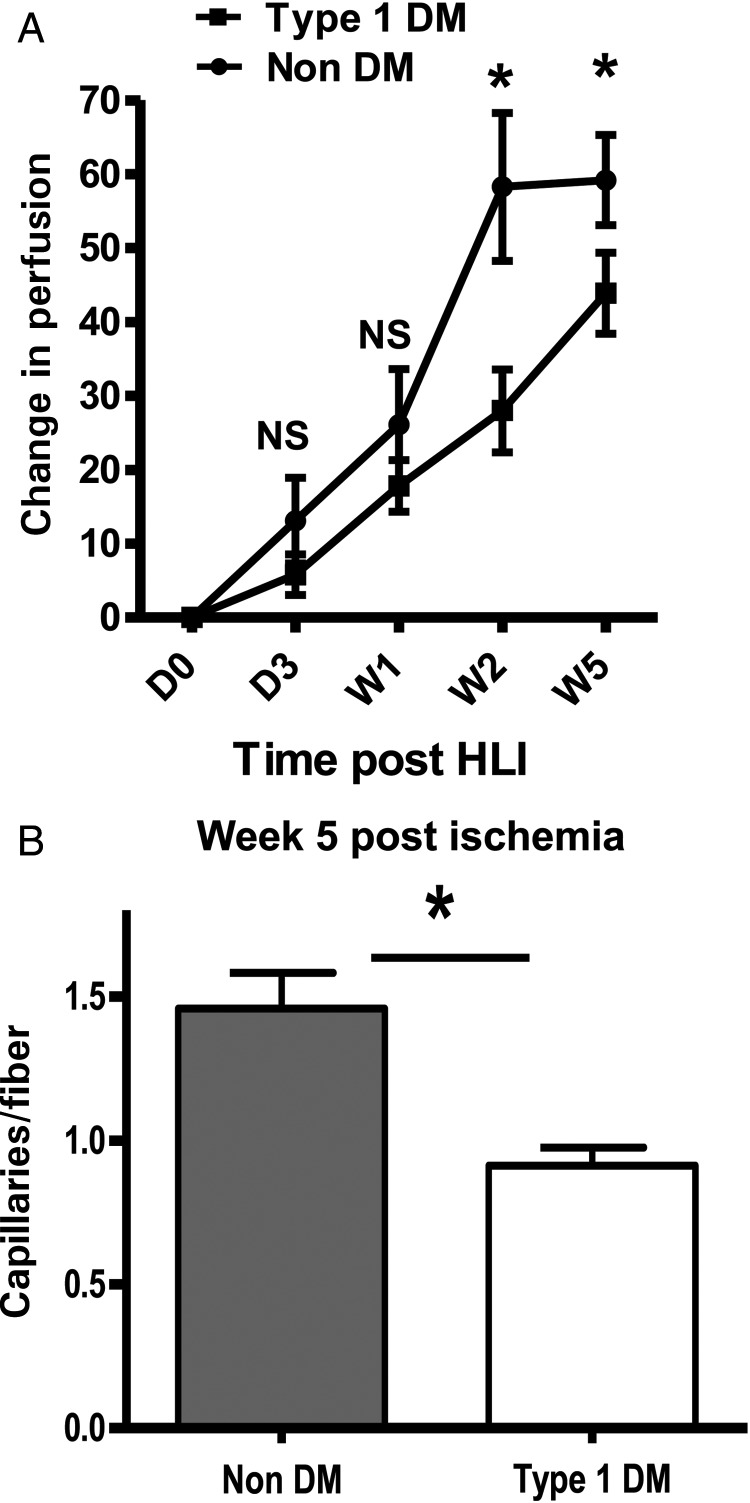
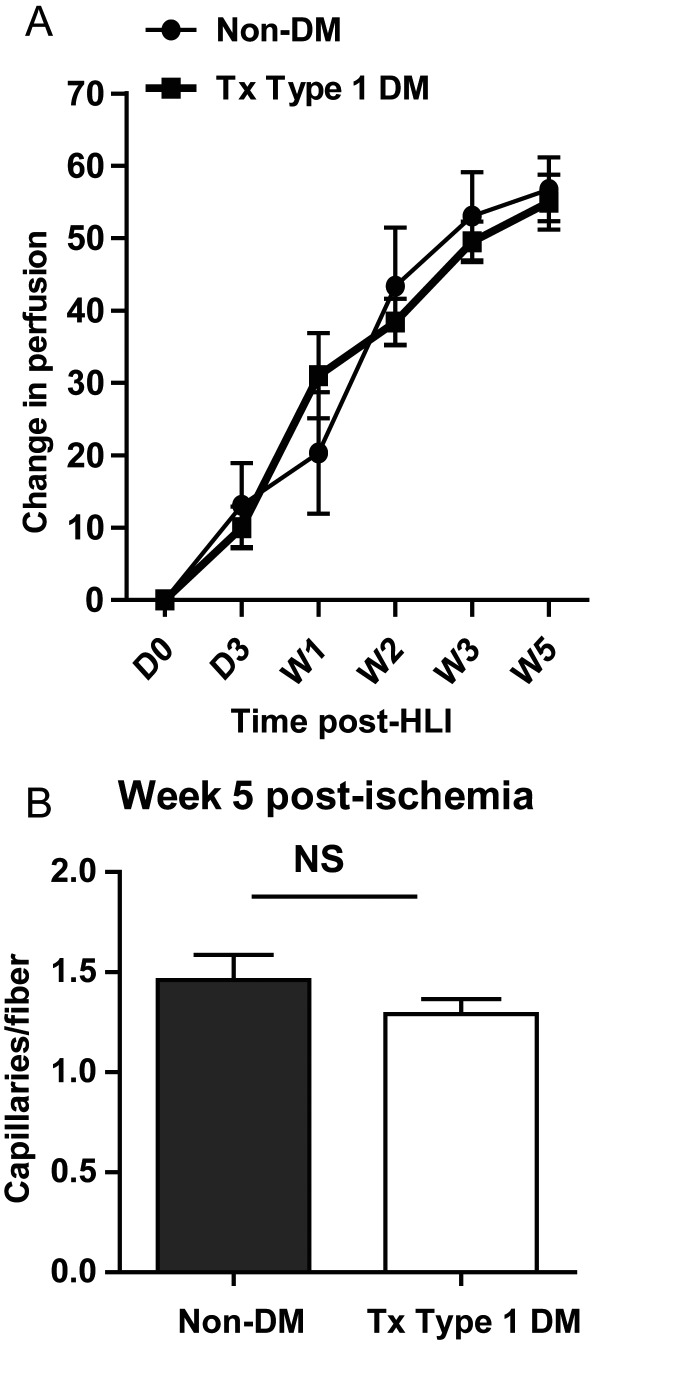
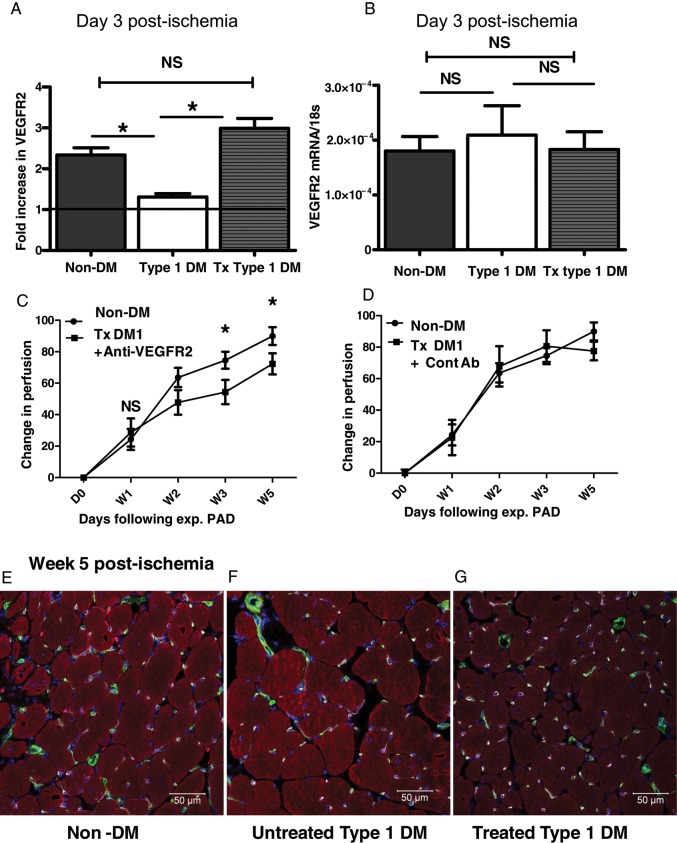
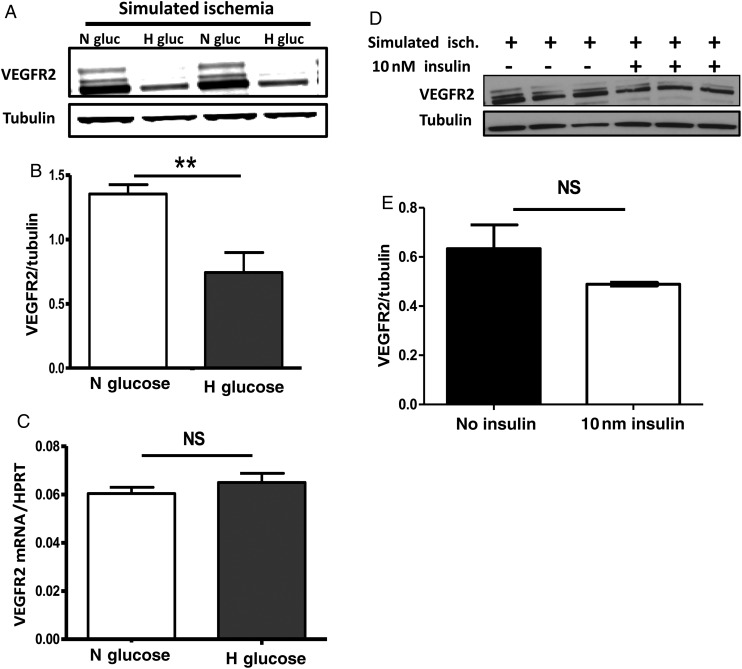
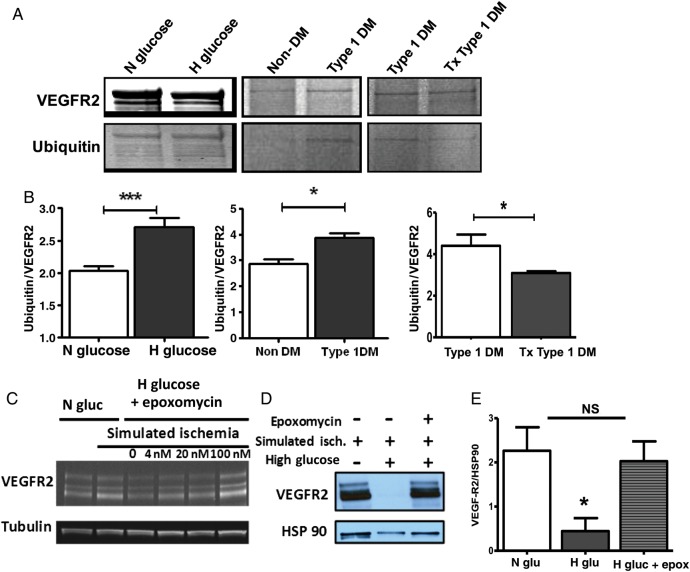
Methods and results: Hind limb ischaemia was induced in non-diabetic, untreated Type 1 DM, and treated Type 1 DM mice. We assessed perfusion recovery, capillary density, VEGFR2 levels, and VEGFR2 ubiquitination in ischaemic hind limbs. We found that untreated Type 1 DM mice showed impaired perfusion recovery, lower hind limb capillary density 5 weeks post-ischaemia, and lower VEGFR2 protein in Day 3 post-ischaemic hind limbs when compared with non-DM controls. Treated Type 1 DM mice had perfusion recovery, capillary density, and VEGFR2 protein levels comparable with that of non-diabetic mice at the same time points. Treatment with anti-VEGFR2 antibody negated that the improved perfusion recovery displayed by treated Type 1 DM mice. In ischaemic Type 1 DM hind limbs and endothelial cells exposed to simulated ischaemia, high glucose impaired VEGFR2 expression and was associated with increased VEGFR2 ubiquitination. Inhibition of the ubiquitin-proteasome complex restored normal endothelial VEGFR2 expression in simulated ischaemia.
Conclusion: Hyperglycaemia in Type 1 DM impairs VEGFR2 protein expression in ischaemic hind limbs, likely due to increased ubiquitination and degradation by the proteasome complex. Glycaemic control allows normal levels of VEGFR2 in ischaemia and improved perfusion recovery.
Keywords: Diabetes; Glycaemic control; Hyperglycaemia; Peripheral arterial disease; Proteasome; VEGF receptor.
Figures

References
-
- Melton LJ, Macken KM, Palumbo PJ, Elveback LR. Incidence and prevalence of clinical peripheral vascular disease in a population-based cohort of diabetic patients. Diabetes Care. 1980;3:650–654. - PubMed
-
- Welborn TA, Knuiman M, McCann V, Stanton K, Constable IJ. Clinical macrovascular disease in Caucasoid diabetic subjects: logistic regression analysis of risk variables. Diabetologia. 1984;27:568–573. - PubMed
-
- Selvin E, Wattanakit K, Steffes MW, Coresh J, Sharrett AR. HbA1c and peripheral arterial disease in diabetes. Diabetes Care. 2006;29:877–882. - PubMed
-
- Jude EB, Eleftheriadou I, Tentolouris N. Peripheral arterial disease in diabetes—a review. Diabetic Med. 2010;27:4–14. - PubMed
-
- UKPDS Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33) The Lancet. 1998;352:837–853. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
