

Postulating a role for connective tissue elements in inferior oblique muscle overaction (an American Ophthalmological Society thesis)
- PMID: 24385670
- PMCID: PMC3812716
Postulating a role for connective tissue elements in inferior oblique muscle overaction (an American Ophthalmological Society thesis)
Abstract
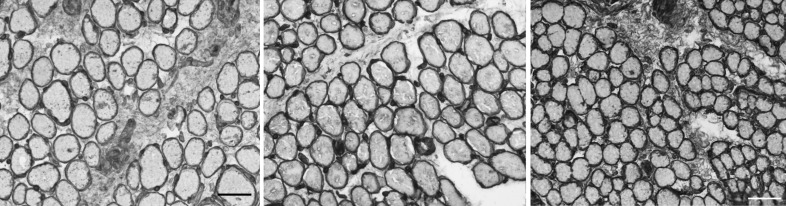
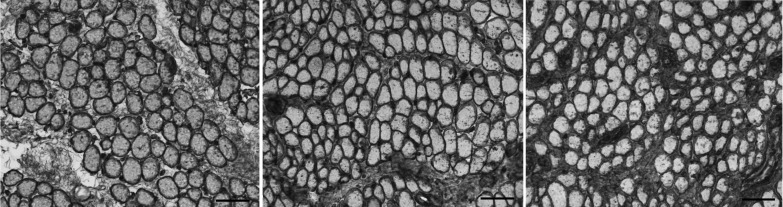
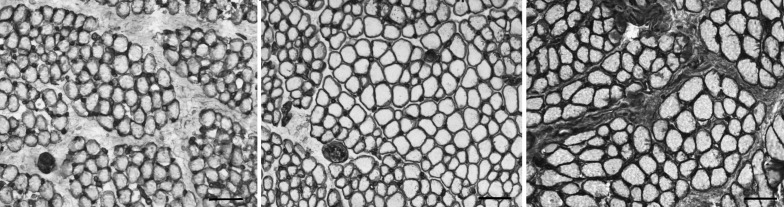
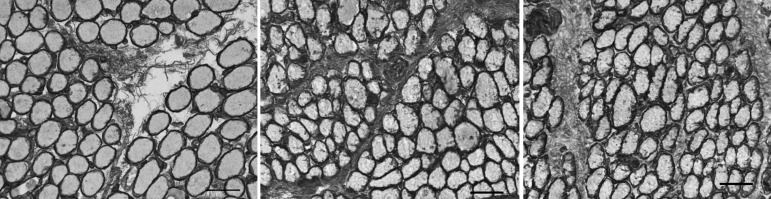
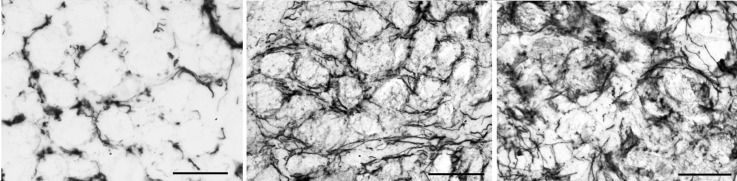
Purpose: To compare the localization and density of collagens I, IV, VI, and elastin, the major protein components of connective tissue, in the inferior oblique muscle of patients with overelevation in adduction and in controls and to characterize changes that develop following surgery. Biomechanical studies suggest that the connective tissue matrix plays a critical role in extraocular muscle function, determining tensile strength and force transmission during contraction.
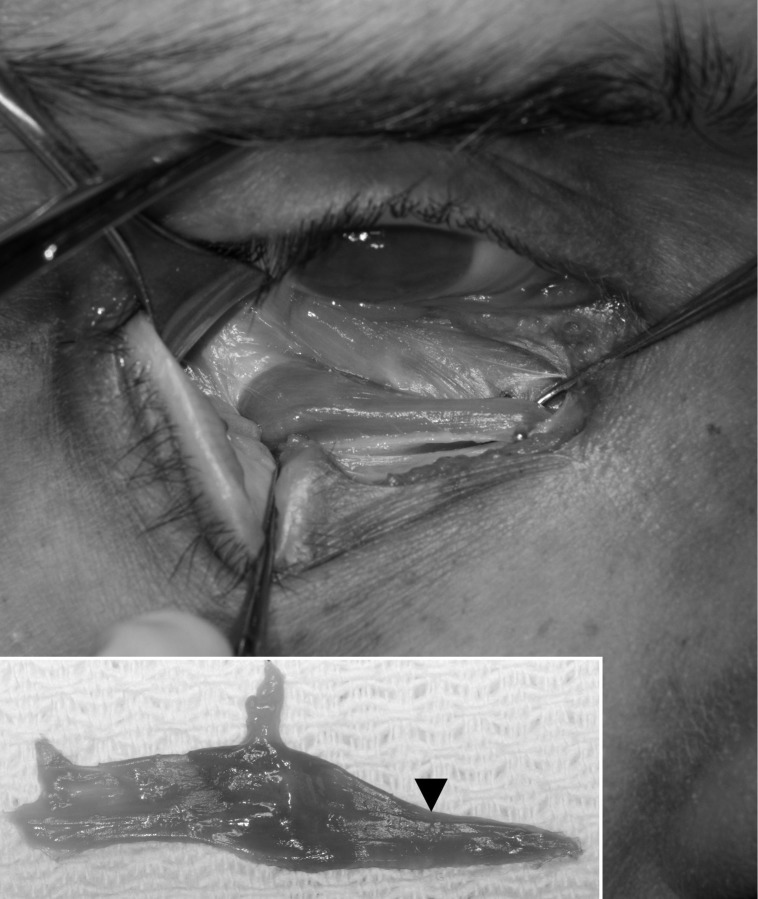
Methods: Prospective laboratory-based case-control study of inferior oblique muscle specimens from 31 subjects: 16 with primary inferior oblique overaction, 6 with craniofacial dysostosis, and 9 normal controls. Collagen I, IV, VI, and elastin were localized and quantified using immunohistochemical staining. Densities were compared using analysis of variance and post hoc comparisons.
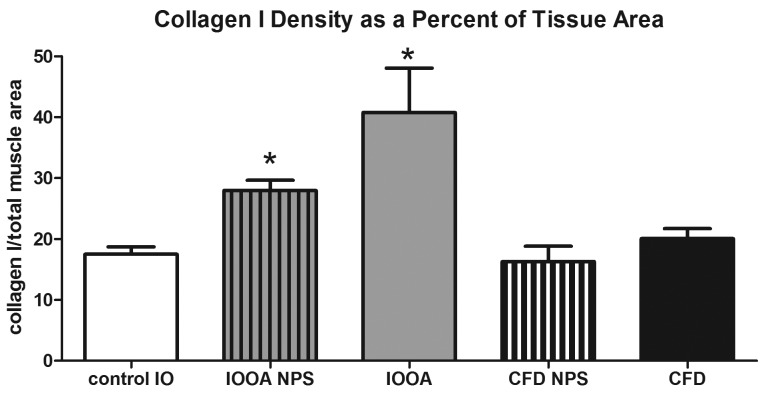
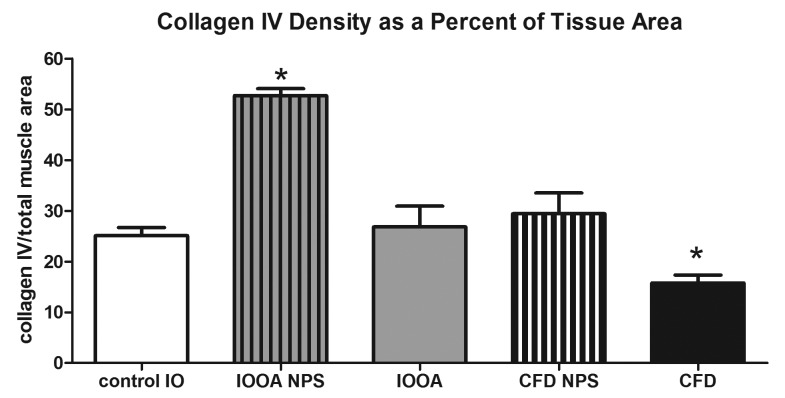
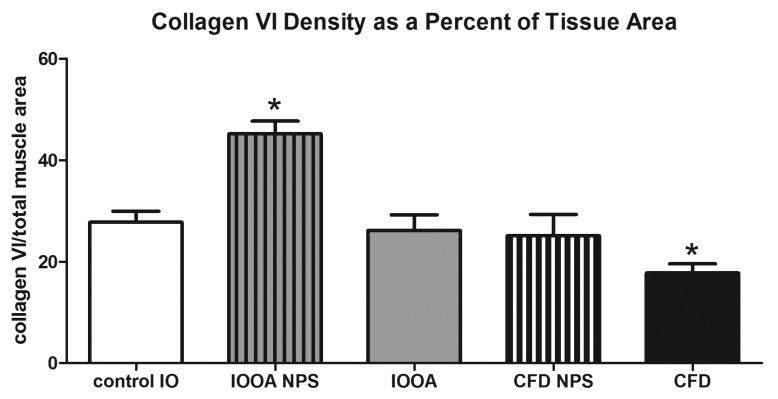
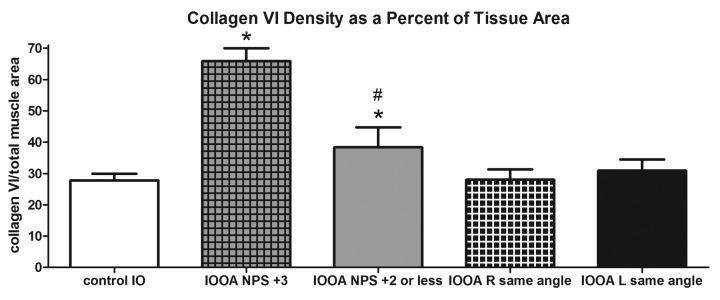
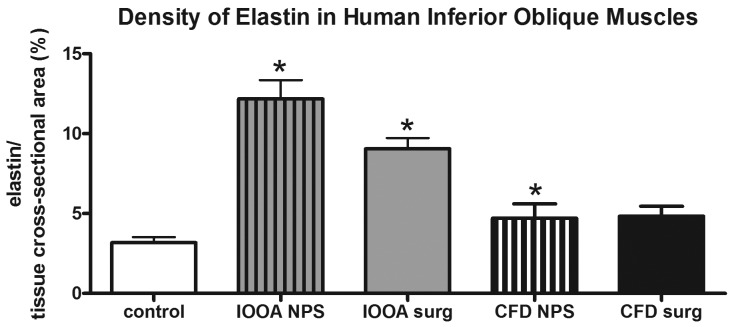
Results: In primary inferior oblique overaction, all connective tissue components in unoperated specimens were elevated compared to controls (P<.0001). Previously operated muscles showed normal levels of collagens IV and VI (P>.27) but increased collagen I. In unoperated craniofacial dysostosis specimens, only elastin was elevated (P=.03), whereas density of collagens IV and VI was lower in previously operated vs unoperated specimens (P=.015).
Conclusions: Elevated collagen and elastin levels in the cohort with primary inferior oblique overaction are consistent with the clinical finding of muscle stiffness. Contrarily, normal connective tissue densities in craniofacial dysostosis support the hypothesis that overelevation in this group reflects anomalous muscle vectors rather than tissue changes. Surgical intervention was associated with changes in the connective tissue matrix in both cohorts. These results have ramifications for treating patients with overelevation in adduction.
Figures
References
-
- Kushner BJ. Multiple mechanisms of extraocular muscle “overaction”. Arch Ophthalmol. 2006;124(5):680–688. - PubMed
-
- Kushner BJ. Incomitant strabismus: Does extraocular muscle form denote function? Arch Ophthalmol. 2010;128(12):1604–1609. - PubMed
-
- Von Noorden GK. Atlas of Strabismus. 4th ed. StLouis: CV Mosby Co; 1983.
-
- Hertle RW, National Eye Institute Sponsored Classification of Eye Movement Abnormalities and Strabismus Working Group A next step in naming and classification of eye movement disorders and strabismus. J AAPOS. 2002;6(4):201–202. - PubMed
-
- American Academy of Ophthalmology . Pediatric Ophthalmology and Strabismus. San Francisco: American Academy of Ophthalmology; 2006.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
