

Optimal duration of fluorouracil-based adjuvant chemotherapy for patients with resectable gastric cancer
- PMID: 24386161
- PMCID: PMC3873471
- DOI: 10.1371/journal.pone.0083196
Optimal duration of fluorouracil-based adjuvant chemotherapy for patients with resectable gastric cancer
Abstract
Background: Although several clinical trials have suggested that postoperative adjuvant chemotherapy can improve survival of patients with gastric cancer, the optimal treatment duration has not been studied. This retrospective analysis evaluated the outcomes of patients with gastric cancer treated with six cycles of fluorouracil-based treatment compared with a cohort treated with four or eight cycles.
Methods: We retrospectively identified 237 patients with stage IB-IIIC gastric cancer who received four, six, or eight cycles of fluorouracil-based adjuvant chemotherapy administered every 3 weeks after radical gastrectomy. The endpoint was overall survival (OS). Factors associated with prognosis were also analyzed.
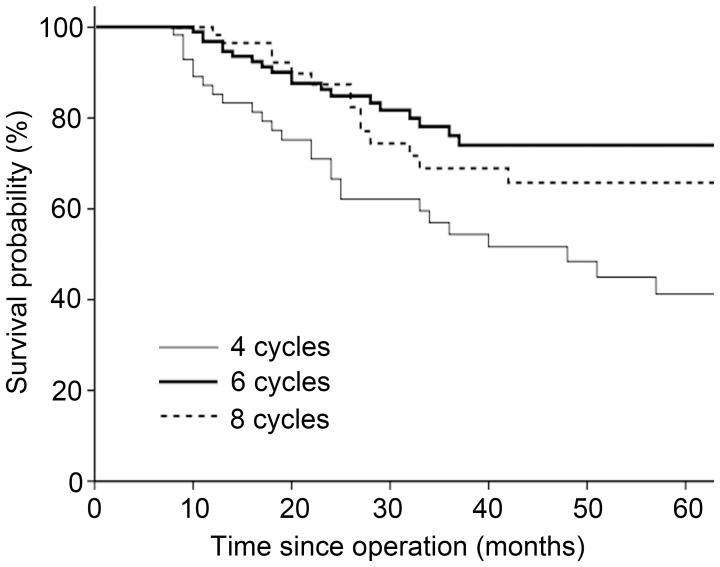
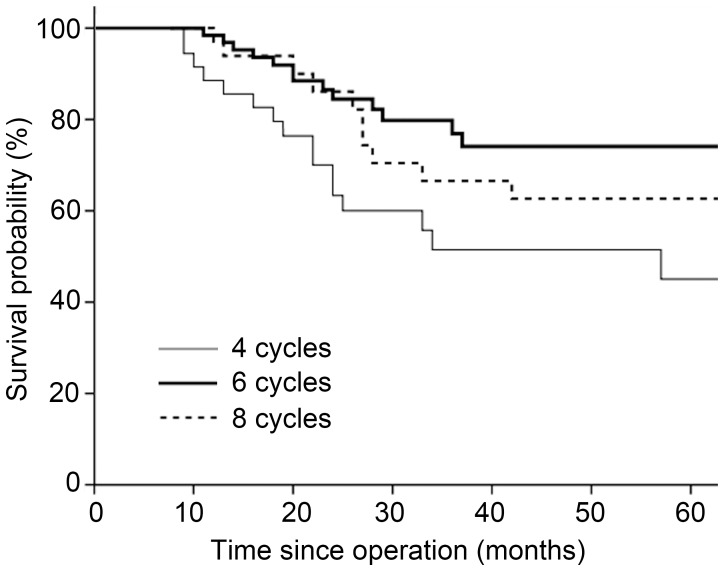
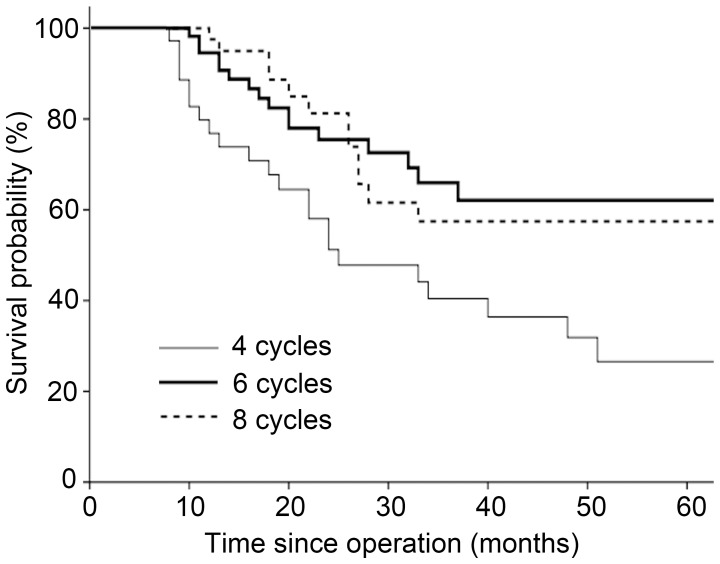
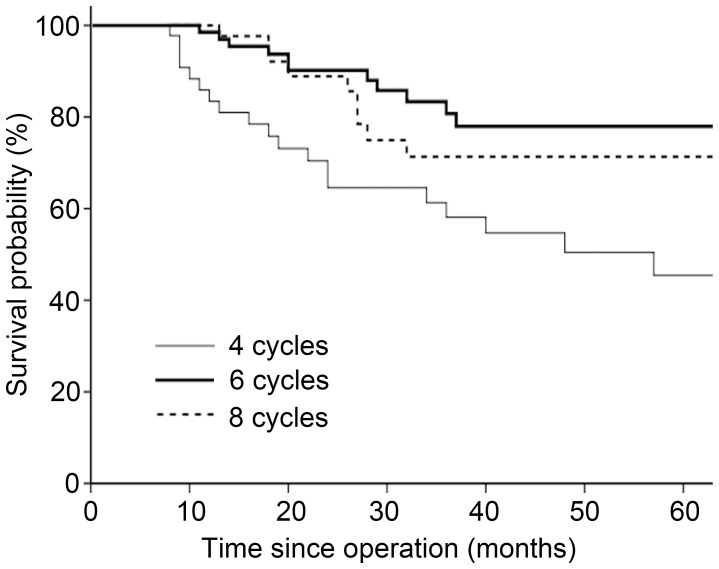
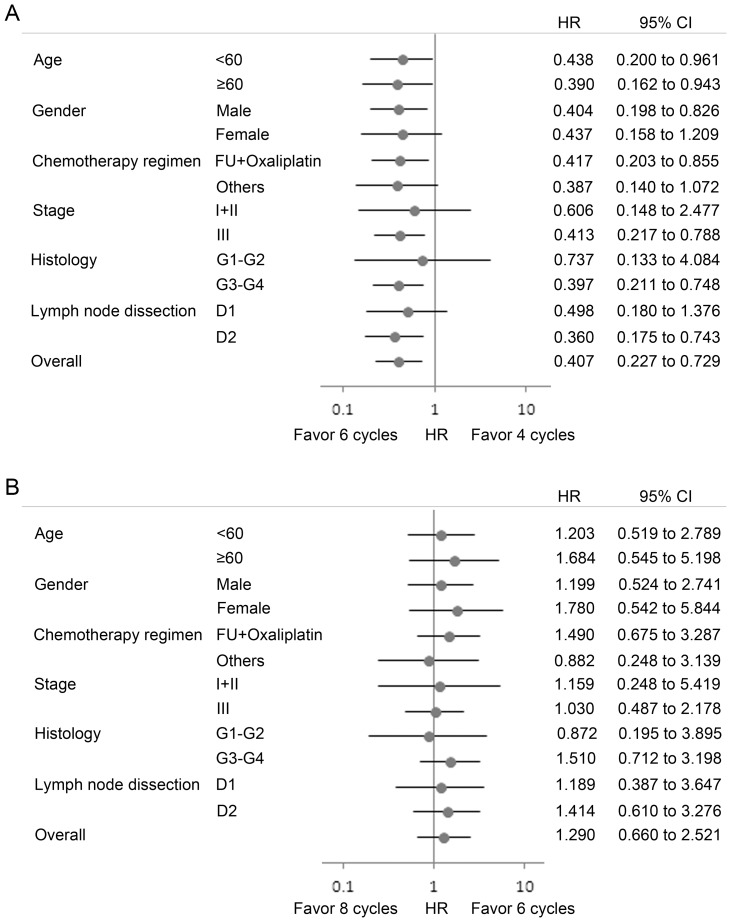
Results: The estimated 3-year OS rates for the four-, six-, and eight-cycle cohorts were 54.4%, 76.1%, and 68.9%, respectively; and the estimated 5-year OS rates were 41.2%, 74.0%, and 65.8%, respectively. Patients who received six cycles were more likely to have a better OS than those who received four cycles (P = 0.002). Eight cycles failed to show an additional survival benefit (P = 0.454). In the multivariate analysis, the number of chemotherapy cycles was associated with OS independent of clinical covariates (P<0.05). Subgroup analysis suggested that among patients in all age groups examined, male patients, and subgroups of fluorouracil plus oxaliplatin combined chemotherapy, stage III, poor differentiation, and gastrectomy with D2 lymphadenectomy, six cycles of adjuvant chemotherapy were associated with a statistically significant benefit of OS compared with four cycles (P<0.05).
Conclusions: Six cycles of adjuvant chemotherapy might lead to a favorable outcome for patients with gastric cancer, and two further cycles could not provide an additional clinical benefit.
Conflict of interest statement
Figures
References
-
- Van Cutsem E, Dicato M, Geva R, Arber N, Bang Y, et al. (2011) The diagnosis and management of gastric cancer: expert discussion and recommendations from the 12th ESMO/World Congress on Gastrointestinal Cancer, Barcelona, 2010. Ann Oncol 22 Suppl 5: v1–9. - PubMed
-
- Sasako M, Sakuramoto S, Katai H, Kinoshita T, Furukawa H, et al. (2011) Five-year outcomes of a randomized phase III trial comparing adjuvant chemotherapy with S-1 versus surgery alone in stage II or III gastric cancer. J Clin Oncol 29: 4387–4393. - PubMed
-
- Bang YJ, Kim YW, Yang HK, Chung HC, Park YK, et al. (2012) Adjuvant capecitabine and oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): a phase 3 open-label, randomised controlled trial. Lancet 379: 315–321. - PubMed
-
- GASTRIC (Global Advanced/Adjuvant Stomach Tumor Research International Collaboration) Group (2010) Paoletti X, Oba K, Burzykowski T, Michiels S, et al. (2010) Benefit of adjuvant chemotherapy for resectable gastric cancer: a meta-analysis. JAMA 303: 1729–1737. - PubMed
-
- Cunningham D, Allum WH, Stenning SP, Thompson JN, Van de Velde CJ, et al. (2006) Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med 355: 11–20. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
