

Five-year follow-up of patients treated for coronary artery disease in the face of an increasing burden of co-morbidity and disease complexity (from the NHLBI Dynamic Registry)
- PMID: 24388624
- PMCID: PMC3946649
- DOI: 10.1016/j.amjcard.2013.10.039
Five-year follow-up of patients treated for coronary artery disease in the face of an increasing burden of co-morbidity and disease complexity (from the NHLBI Dynamic Registry)
Abstract
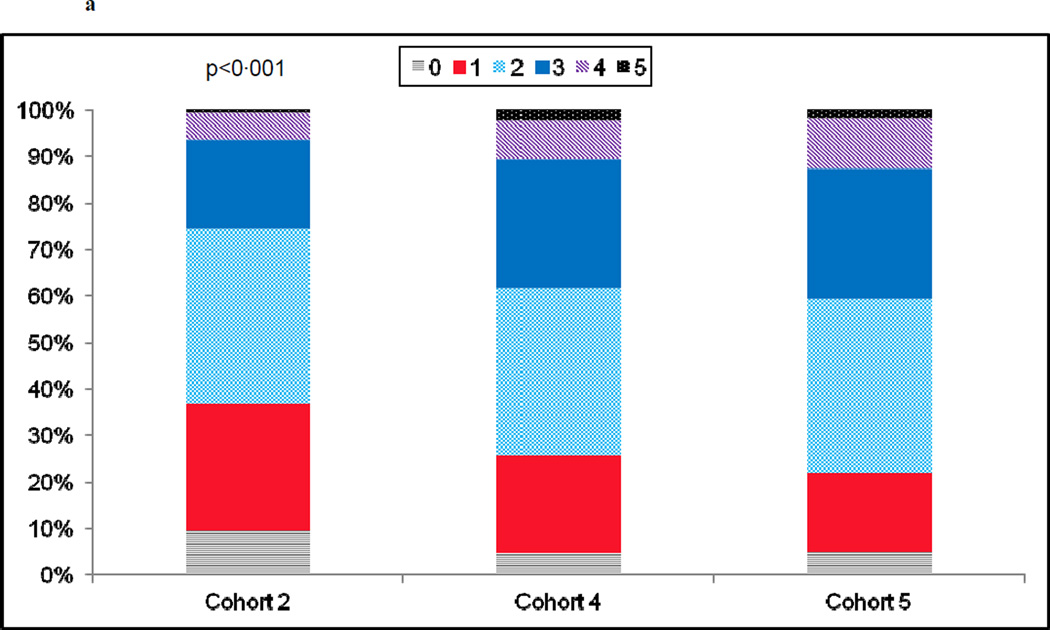
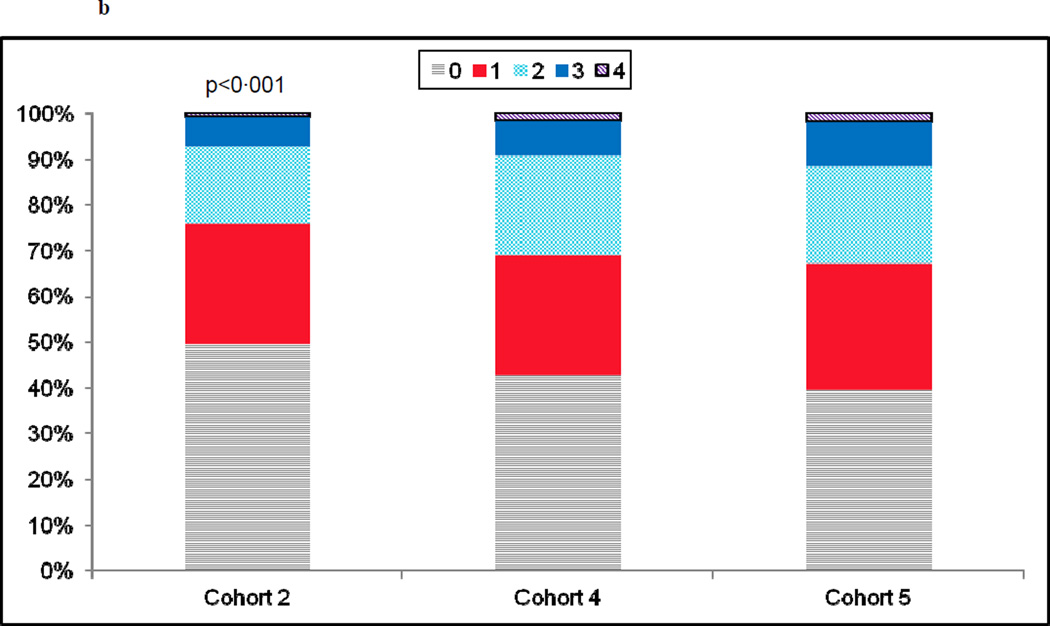
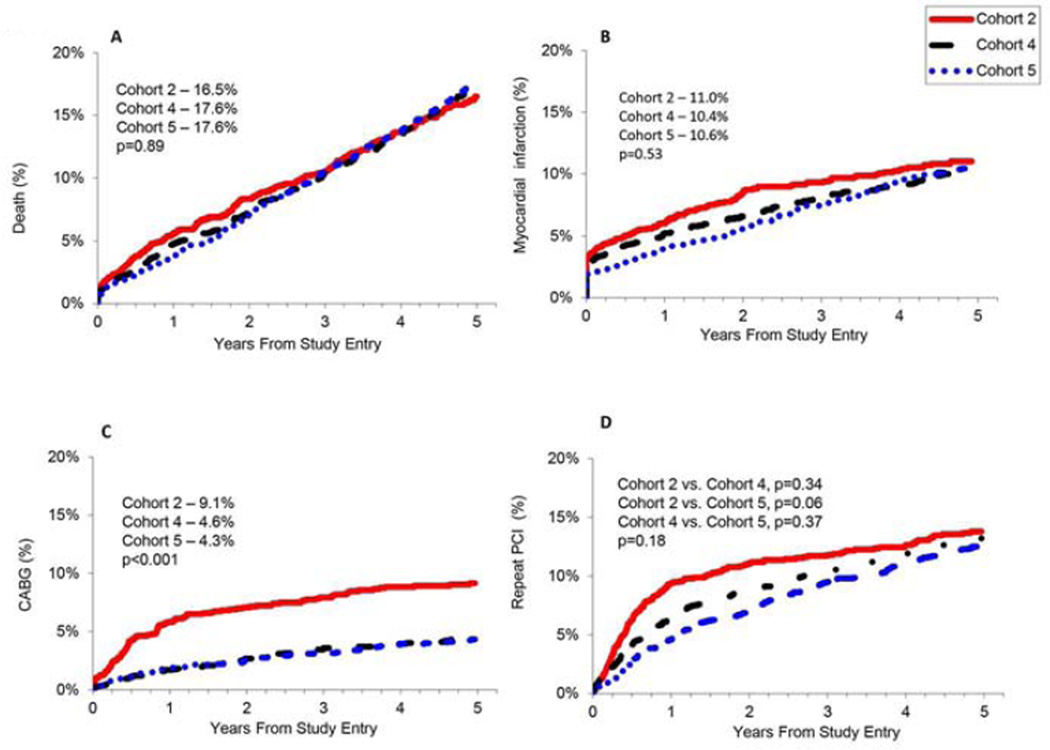
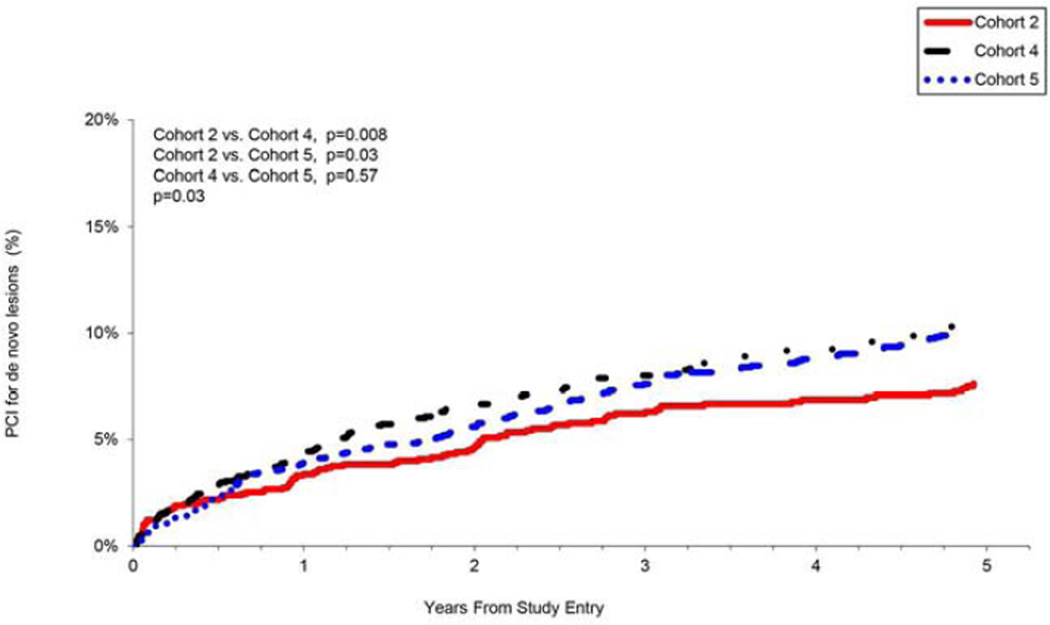
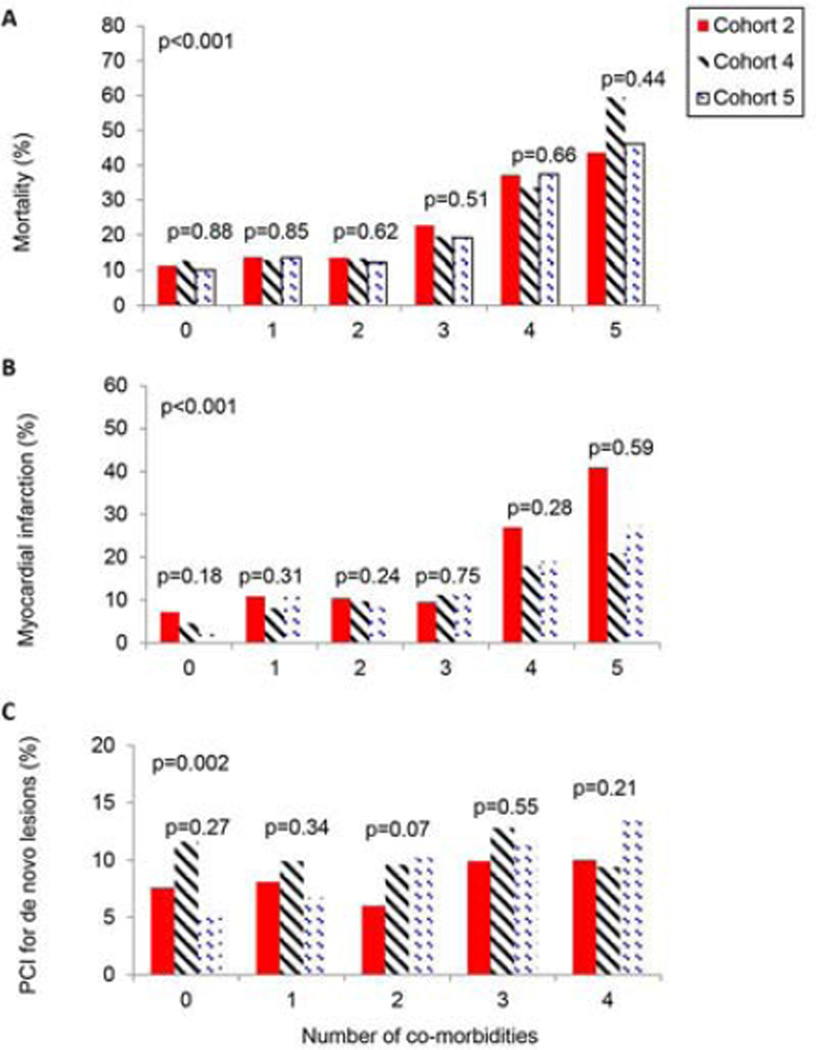
Management of coronary artery disease (CAD) has evolved over the past decade, but there are few prospective studies evaluating long-term outcomes in a real-world setting of evolving technical approaches and secondary prevention. The aim of this study was to determine how the mortality and morbidity of CAD has changed in patients who have undergone percutaneous coronary intervention (PCI), in the setting of co-morbidities and evolving management. The National Heart, Lung, and Blood Institute Dynamic Registry was a cohort study of patients undergoing PCI at various time points. Cohorts were enrolled in 1999 (cohort 2, n = 2,105), 2004 (cohort 4, n = 2,112), and 2006 (cohort 5, n = 2,176), and each was followed out to 5 years. Primary outcomes were death, myocardial infarction (MI), coronary artery bypass grafting, repeat PCI, and repeat revascularization. Secondary outcomes were PCI for new obstructive lesions at 5 years, 5-year rates of death and MI stratified by the severity of coronary artery and co-morbid disease. Over time, patients were more likely to have multiple co-morbidities and more severe CAD. Despite greater disease severity, there was no significant difference in death (16.5% vs 17.6%, adjusted hazard ratio [HR] 0.89, 95% confidence interval [CI] 0.74 to 1.08), MI (11.0% vs 10.6%, adjusted HR 0.87, 95% CI 0.70 to 1.08), or repeat PCI (20.4% vs 22.2%, adjusted HR 0.98, 95% CI 0.85 to 1.17) at 5-year follow-up, but there was a significant decrease in coronary artery bypass grafting (9.1% vs 4.3%, adjusted HR 0.44, 95% CI 0.32 to 0.59). Patients with 5 co-morbidities had a 40% to 60% death rate at 5 years. There was a modestly high rate of repeat PCI for new lesions, indicating a potential failure of secondary prevention for this population in the face of increasing co-morbidity. Overall 5-year rates of death, MI, repeat PCI, and repeat PCI for new lesions did not change significantly in the context of increased co-morbidities and complex disease.
Copyright © 2014 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Fang J, Alderman MH, Keenan NL, Ayala C. Acute myocardial infarction hospitalization in the United States, 1979 to 2005. Am J Med. 2010;123:259–266. - PubMed
-
- Venkitachalam L, Kip KE, Mulukutla SR, Selzer F, Laskey W, Slater J, Cohen HA, Wilensky RL, Williams DO, Marroquin OC, Sutton-Tyrrell K, Bunker CH, Kelsey SF. Temporal trends in patient-reported angina at 1 year after percutaneous coronary revascularization in the stent era: a report from the National Heart, Lung, and Blood Institute-sponsored 1997–2006 dynamic registry. Circ Cardiovasc Qual Outcomes. 2009;2:607–615. - PMC - PubMed
-
- Smith SC, Benjamin EJ, Bonow RO, Braun LT, Creager MA, Franklin BA, Gibbons RJ, Grundy SM, Hiratzka LF, Jones DW, Lloyd-Jones DM, Minissian M, Mosca L, Peterson ED, Sacco RL, Spertus J, Stein JH, Taubert KA. AHA/ACCF Secondary Prevention and Risk Reduction Therapy for Patients With Coronary and Other Atherosclerotic Vascular Disease: 2011 Update: A Guideline From the American Heart Association and American College of Cardiology Foundation. Circulation. 2011;124:2458–2473. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
