

The significance of intraoperative monitoring of muscle motor evoked potentials during unruptured large and giant cerebral aneurysm surgery
- PMID: 24390185
- PMCID: PMC4533417
- DOI: 10.2176/nmc.oa.2013-0001
The significance of intraoperative monitoring of muscle motor evoked potentials during unruptured large and giant cerebral aneurysm surgery
Abstract
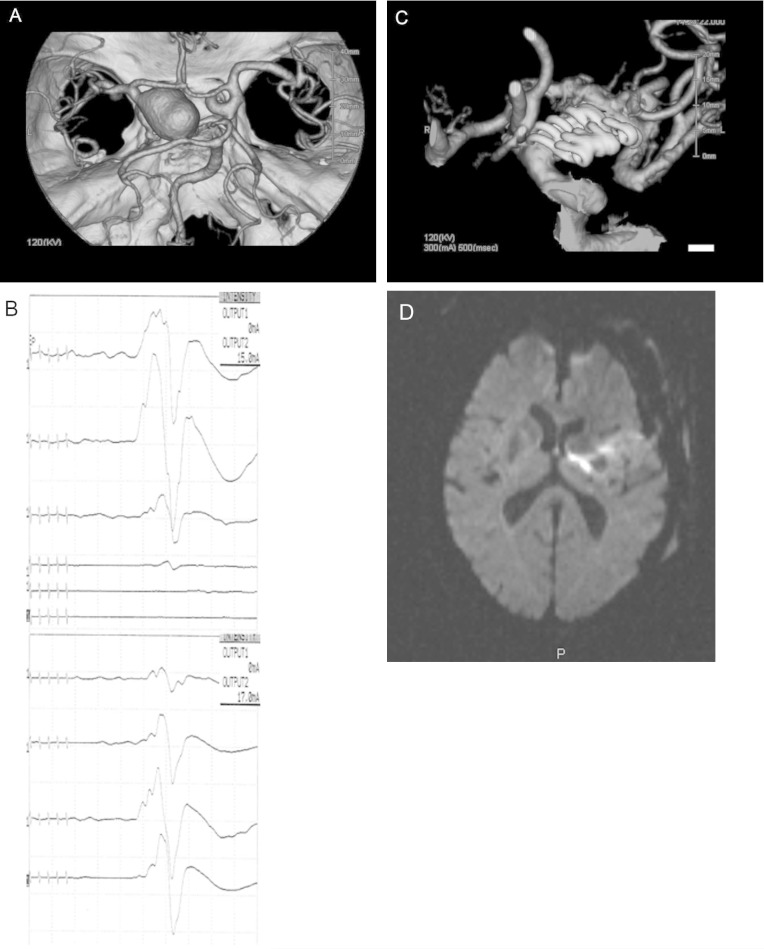
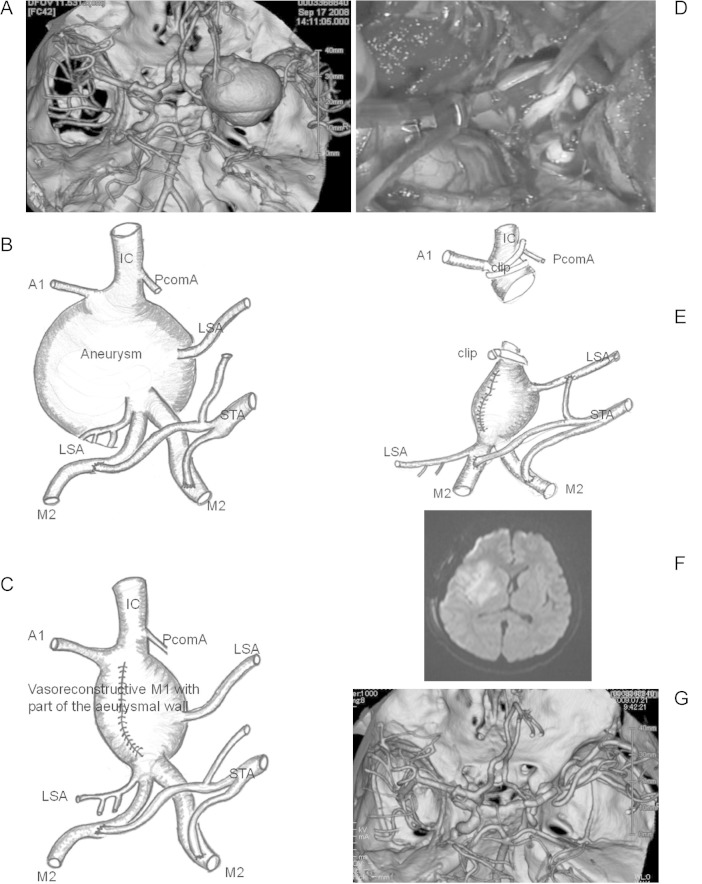
The goal of this study was to characterize the utility of muscle motor evoked potentials (MMEPs) elicited by direct cortical stimulation as a means of monitoring during unruptured large and giant cerebral aneurysm surgery. This analysis focused on intraoperative changes in MMEPs and their relationship to postoperative motor function. The study population consisted of 50 patients who underwent surgery for large (n = 31) or giant (n = 19) cerebral aneurysms. Intraoperative MMEPs were continuously and successfully obtained in muscles belonging to the vascular territory of interest. There was no postoperative motor paresis in 31 (62%) patients in whom intraoperative MMEPs remained unchanged. Transient MMEP change occurred in 15 (30%) of the 50 patients, but 9 of those patients had no postoperative motor deficits, 5 had transient motor deficits, and 1 suffered permanent motor deficits resulting from postoperative delayed blood flow insufficiency due to arteriosclerosis of the parent artery. Permanent MMEP loss occurred in 4 (8%) of 50 patients, all of whom developed severe and permanent postoperative motor deficits. MMEP is a useful monitoring modality in patients undergoing surgery for large or giant cerebral aneurysms. This strategy can help predict functional prognosis or guide the neurosurgeon intraoperatively in an effort to promote better outcomes.
Conflict of interest statement
The authors have no personal, financial, or institutional interest in any of the drugs, materials, or devices described in this article.
Figures
References
-
- Szelényi A, Langer D, Kothbauer K, De Camargo AB, Flamm ES, Deletis V: Monitoring of muscle motor evoked potentials during cerebral aneurysm surgery: intraoperative changes and postoperative outcome. J Neurosurg 105: 675– 681, 2006. - PubMed
-
- Chen L, Lang L, Zhou L, Song D, Mao Y: Bypass or not? Adjustment of surgical strategies according to motor evoked potential changes in large middle cerebral artery aneurysm surgery. World Neurosurg 77: 398.E1– 6, 2012. - PubMed
-
- Friedman WA, Kaplan BL, Day AL, Sypert GW, Curran MT: Evoked potential monitoring during aneurysm operation: observations after fifty cases. Neurosurgery 20: 678– 687, 1987. - PubMed
-
- Guo L, Gelb AW: The use of motor evoked potential monitoring during cerebral aneurysm surgery to predict pure motor deficits due to subcortical ischemia. Clin Neurophysiol 122: 648– 655, 2011. - PubMed
-
- Horiuchi K, Suzuki K, Sasaki T, Matsumoto M, Sakuma J, Konno Y, Oinuma M, Itakura T, Kodama N: Intraoperative monitoring of blood flow insufficiency during surgery of middle cerebral artery aneurysms. J Neurosurg 103: 275– 283, 2005. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical