

Demographic profile and outcome analysis of pediatric intensive care patients
- PMID: 24391412
- PMCID: PMC3876846
Demographic profile and outcome analysis of pediatric intensive care patients
Abstract
Background: Demographic profile and outcome can vary in pediatric intensive care unit (PICU) patients. The aim of our study was to analyze demographic profile and outcome in a Greek PICU.
Methods: Prospective observational study.
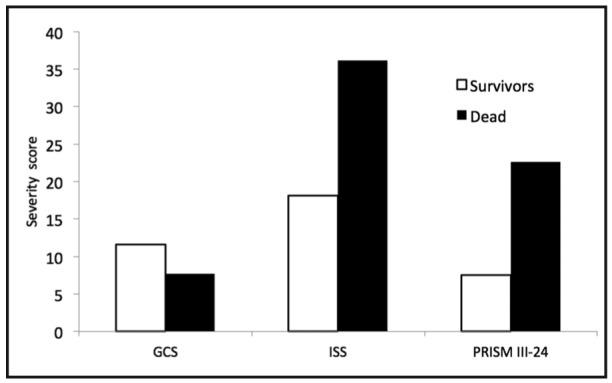
Data collected: demographic profile; co morbidities; source and diagnosis at admission; Pediatric Risk of Mortality (PRISM III-24); Glasgow Coma Scale (GCS, pediatric); Injury Severity Score (ISS); procedures; treatment; mechanical ventilation (MV); MV days; length of stay (LOS) and the outcome at PICU discharge.
Statistical analysis: Student's t-test; Mann-Whitney U test; Kruskall-Wallis test; χ(2) criterion with relative risk (RR) estimation; Cox regression analysis; as appropriate. Values are mean ± SD, p < 0.05.
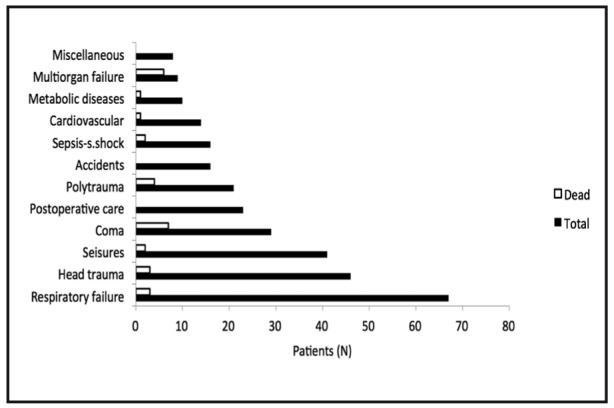
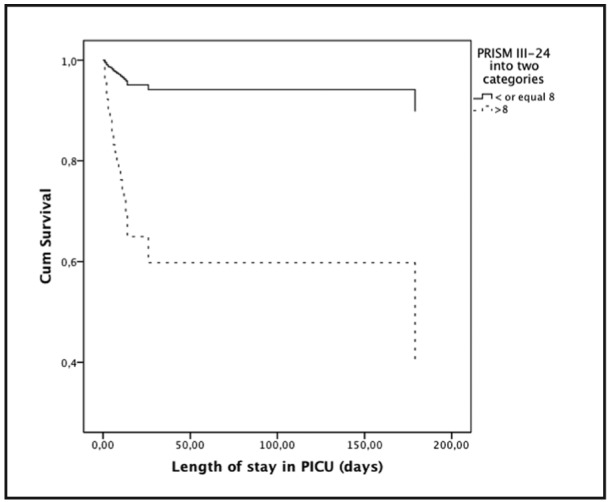
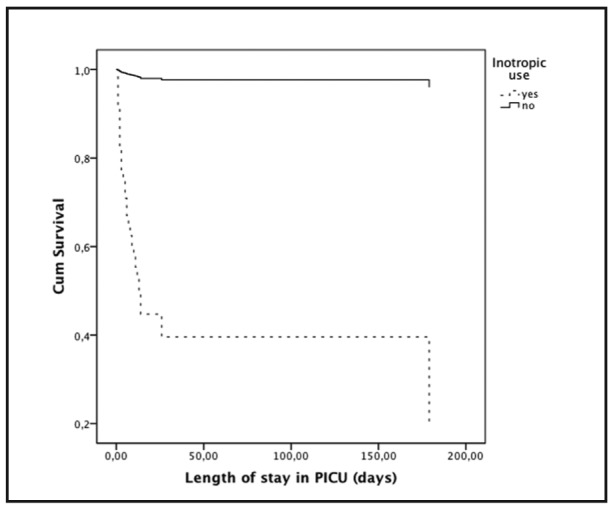
Results: 300 patients (196 boys/104 girls), aged 54.26 ± 49.93 months, were admitted due to respiratory failure (22.3%), head trauma (15.3%), seizures (13.7%), coma (9.7%), postoperative care (7.7%), polytrauma (7%), accidents (5.3%), sepsis-septic shock (5.3%), cardiovascular diseases (4.7%), metabolic diseases (3.3%), multiple organ failure syndrome (3%) and miscellaneous diseases (2.7%). PRISM III-24 score was 8.97 ± 7.79 and predicted mortality rate was 11.16% ± 18.65. MV rate was 67.3% (58.3% at admission) for 6.54 ± 14.45 days, LOS 8.85 ± 23.28 days and actual PICU mortality rate 9.7%. Patients who died had statistically worse severity scores. Significant mortality risk factors were inotropic use, PRISM III-24 > 8, MV, arterial and central venous catheterization, nosocomial infections, complications, and cancer. COX regression analysis showed that PRISM III-24 score and inotropic use were independent predictors of mortality.
Conclusions: Demographic profile followed similar patterns to relevant studies while there were major differences in case mix and the severity of the disease. Mortality rate (9.7%) was relatively high but better than predicted and in accordance with the characteristics of our population.
Keywords: mortality; mortality risk factors; pediatric intensive care unit; pediatric risk of mortality PRISM III-24.
Figures
References
-
- Forrest BC, Shipman AS, Dougherty D, Miller RM. Outcome research in pediatric settings: Recent trends and future directions. Pediatrics. 2003;111:171–178. - PubMed
-
- Bennett NR. Paediatric intensive care. Br J Anaesth. 1999;83:139–156. - PubMed
-
- Epstein D, Brill JE. A history of pediatric critical care medicine. Pediatr Res. 2005;58:987–996. - PubMed
-
- Pollack MM, Cuerdon TT, Patel KM, Ruttimann UE, Getson PR, Levetown M. Impact of quality-of-care factors on pediatric intensive care unit mortality. Jama. 1994;272:941–946. - PubMed
-
- Pollack MM, Patel KM, Ruttimann E. Pediatric critical care training programs have a positive effect on pediatric intensive care mortality. Crit Care Med. 1997;25:1637–1642. - PubMed
LinkOut - more resources
Full Text Sources