

Effect of erythropoiesis-stimulating agents on blood pressure in pre-dialysis patients
- PMID: 24391978
- PMCID: PMC3877353
- DOI: 10.1371/journal.pone.0084848
Effect of erythropoiesis-stimulating agents on blood pressure in pre-dialysis patients
Abstract
Introduction: Erythropoiesis-Stimulating Agents (ESA) are hypothesized to increase cardiovascular mortality in patients with chronic kidney disease. One of the proposed mechanisms is the elevation of blood pressure (BP) by ESA. Therefore, we aimed to determine whether the use of ESA was associated with antihypertensive treatment and higher BP.
Materials and methods: In this cohort 502 incident pre-dialysis patients were included who started specialized pre-dialysis care in 25 clinics in the Netherlands. Data on medication including ESA use and dose, co-morbidities and BP were routinely collected every 6 months. Antihypertensive treatment and BP were compared for patients with and without ESA at baseline. Differences in antihypertensive medication and BP during pre-dialysis care were estimated with linear mixed models adjusted for age, sex, body mass index, cardiovascular disease, diabetes mellitus and estimated glomerular filtration rate.
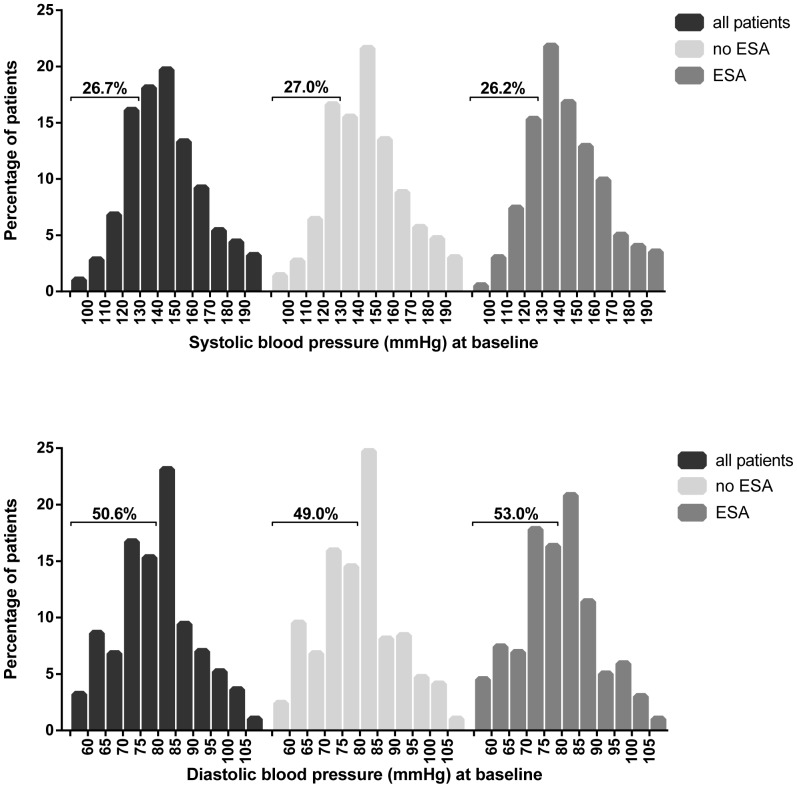
Results: At baseline, 95.6% of patients with ESA were treated with antihypertensive medication and 73.1% of patients without ESA. No relevant difference in BP was found. During pre-dialysis care patients with ESA used 0.77 (95% CI 0.63;0.91) more classes of antihypertensive drugs. The adjusted difference in systolic blood pressure (SBP) was -0.3 (95% CI -2.7;2.0) mmHg and in diastolic blood pressure (DBP) was -1.0 (95% CI -2.1;0.3) mmHg for patients with ESA compared to patients without ESA. Adjusted SBP was 3.7 (95% CI -1.6;9.0) mmHg higher in patients with a high ESA dose compared to patients with a low ESA dose.
Conclusions: Our study confirms the hypertensive effect of ESA, since ESA treated patients received more antihypertensive agents. However, no relevant difference in BP was found between patients with and without ESA, thus the increase in BP seems to be controlled for by antihypertensive medication.
Conflict of interest statement
Figures
Similar articles
-
Treatment with high dose of erythropoiesis-stimulating agents and mortality: analysis with a sequential Cox approach and a marginal structural model.Pharmacoepidemiol Drug Saf. 2015 Oct;24(10):1068-75. doi: 10.1002/pds.3855. Epub 2015 Aug 12. Pharmacoepidemiol Drug Saf. 2015. PMID: 26265483
-
Impact of higher hemoglobin targets on blood pressure and clinical outcomes: a secondary analysis of CHOIR.Nephrol Dial Transplant. 2012 Sep;27(9):3606-14. doi: 10.1093/ndt/gfs123. Epub 2012 May 9. Nephrol Dial Transplant. 2012. PMID: 22573238 Free PMC article. Clinical Trial.
-
Blood pressure and antihypertensive medication profile in a multiethnic Asian population of stable chronic kidney disease patients.Singapore Med J. 2016 May;57(5):267-73. doi: 10.11622/smedj.2016089. Singapore Med J. 2016. PMID: 27212015 Free PMC article.
-
Effects of blood-pressure-lowering treatment on outcome incidence in hypertension: 10 - Should blood pressure management differ in hypertensive patients with and without diabetes mellitus? Overview and meta-analyses of randomized trials.J Hypertens. 2017 May;35(5):922-944. doi: 10.1097/HJH.0000000000001276. J Hypertens. 2017. PMID: 28141660 Review.
-
Treatment of Hypertension: Which Goal for Which Patient?Adv Exp Med Biol. 2017;956:117-127. doi: 10.1007/5584_2016_97. Adv Exp Med Biol. 2017. PMID: 27722961 Review.
Cited by
-
Genes critical for development and differentiation of dopaminergic neurons are downregulated in Parkinson's disease.J Neural Transm (Vienna). 2023 Apr;130(4):495-512. doi: 10.1007/s00702-023-02604-x. Epub 2023 Feb 23. J Neural Transm (Vienna). 2023. PMID: 36820885
-
The Safety of Erythropoiesis-Stimulating Agents for the Treatment of Anemia Resulting from Chronic Kidney Disease.Clin Drug Investig. 2016 Jun;36(6):421-31. doi: 10.1007/s40261-016-0378-y. Clin Drug Investig. 2016. PMID: 26894799 Review.
-
Effects of Erythropoietin-Stimulating Agents on Blood Pressure in Patients with Non-Dialysis CKD and Renal Anemia.Kidney Dis (Basel). 2020 Jul;6(4):299-308. doi: 10.1159/000507396. Epub 2020 Jun 12. Kidney Dis (Basel). 2020. PMID: 32903814 Free PMC article.
-
Low Urinary Creatinine Excretion Is Associated With Self-Reported Frailty in Patients With Advanced Chronic Kidney Disease.Kidney Int Rep. 2017 Mar 10;2(4):676-685. doi: 10.1016/j.ekir.2017.02.021. eCollection 2017 Jul. Kidney Int Rep. 2017. PMID: 29142985 Free PMC article.
References
-
- Muntner P, Anderson A, Charleston J, Chen Z, Ford V, et al. (2010) Hypertension awareness, treatment, and control in adults with CKD: results from the Chronic Renal Insufficiency Cohort (CRIC) Study. Am J Kidney Dis 55: 441–451 S0272-6386(09)01263-3 [pii];10.1053/j.ajkd.2009.09.014 [doi] - DOI - PMC - PubMed
-
- Buckalew VM Jr, Berg RL, Wang SR, Porush JG, Rauch S, et al... (1996) Prevalence of hypertension in 1,795 subjects with chronic renal disease: the modification of diet in renal disease study baseline cohort. Modification of Diet in Renal Disease Study Group. Am J Kidney Dis 28: 811–821. S0272638696002363 [pii]. - PubMed
-
- Sarnak MJ, Levey AS (2003) Schoolwerth AC, Coresh J, Culleton B, et al (2003) Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Hypertension 42: 1050–1065 10.1161/01.HYP.0000102971.85504.7c [doi];42/5/1050 [pii] - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
