

Meditation programs for psychological stress and well-being: a systematic review and meta-analysis
- PMID: 24395196
- PMCID: PMC4142584
- DOI: 10.1001/jamainternmed.2013.13018
Meditation programs for psychological stress and well-being: a systematic review and meta-analysis
Abstract
Importance: Many people meditate to reduce psychological stress and stress-related health problems. To counsel people appropriately, clinicians need to know what the evidence says about the health benefits of meditation.
Objective: To determine the efficacy of meditation programs in improving stress-related outcomes (anxiety, depression, stress/distress, positive mood, mental health-related quality of life, attention, substance use, eating habits, sleep, pain, and weight) in diverse adult clinical populations.
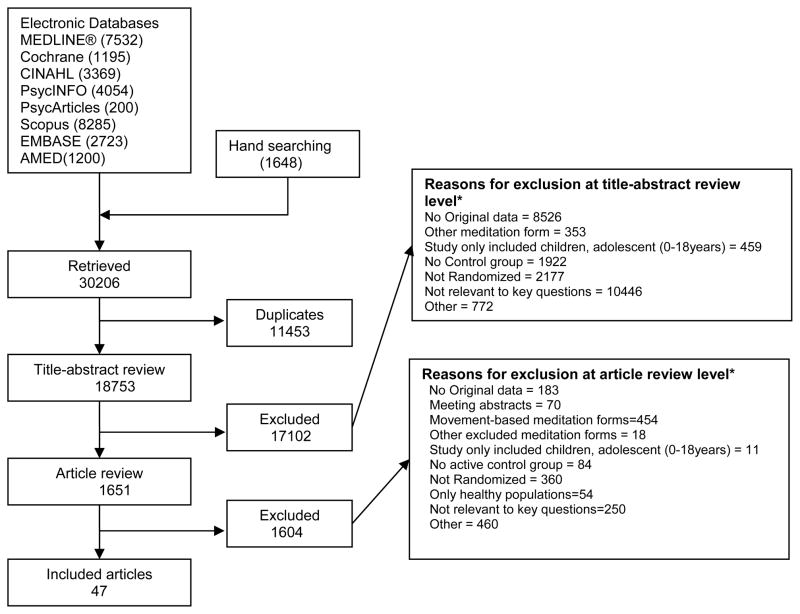
Evidence review: We identified randomized clinical trials with active controls for placebo effects through November 2012 from MEDLINE, PsycINFO, EMBASE, PsycArticles, Scopus, CINAHL, AMED, the Cochrane Library, and hand searches. Two independent reviewers screened citations and extracted data. We graded the strength of evidence using 4 domains (risk of bias, precision, directness, and consistency) and determined the magnitude and direction of effect by calculating the relative difference between groups in change from baseline. When possible, we conducted meta-analyses using standardized mean differences to obtain aggregate estimates of effect size with 95% confidence intervals.
Findings: After reviewing 18 753 citations, we included 47 trials with 3515 participants. Mindfulness meditation programs had moderate evidence of improved anxiety (effect size, 0.38 [95% CI, 0.12-0.64] at 8 weeks and 0.22 [0.02-0.43] at 3-6 months), depression (0.30 [0.00-0.59] at 8 weeks and 0.23 [0.05-0.42] at 3-6 months), and pain (0.33 [0.03- 0.62]) and low evidence of improved stress/distress and mental health-related quality of life. We found low evidence of no effect or insufficient evidence of any effect of meditation programs on positive mood, attention, substance use, eating habits, sleep, and weight. We found no evidence that meditation programs were better than any active treatment (ie, drugs, exercise, and other behavioral therapies).
Conclusions and relevance: Clinicians should be aware that meditation programs can result in small to moderate reductions of multiple negative dimensions of psychological stress. Thus, clinicians should be prepared to talk with their patients about the role that a meditation program could have in addressing psychological stress. Stronger study designs are needed to determine the effects of meditation programs in improving the positive dimensions of mental health and stress-related behavior.
Figures
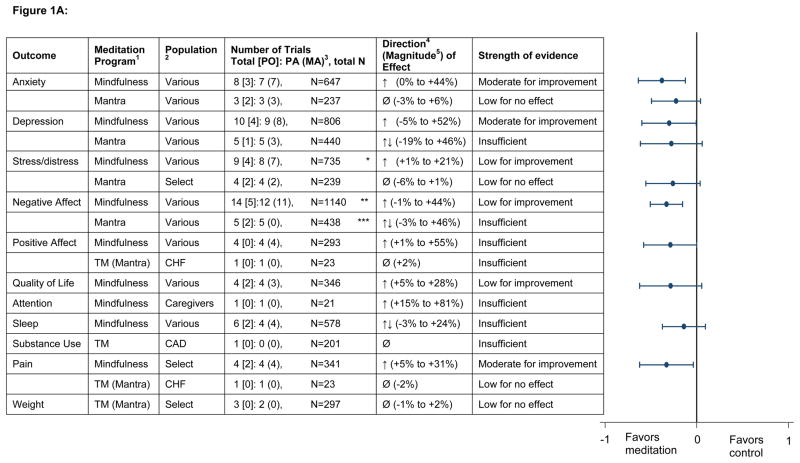
CSM = Clinically Standardized Meditation, a mantra meditation program; TM=Transcendental Meditation, a mantra meditation program
CHF = Congestive Heart Failure; CAD = Coronary Artery Disease
PO = Number of trials in which this was a primary outcome for the trial; PA = Primary Analysis; MA = Meta-analysis; N = sample size
Direction based on relative difference in change analysis:
↑ indicates that the meditation group improved relative to the control group (with a relative difference generally greater than or equal to 5 percent across trials).
↓ indicates the meditation group worsened relative to the control group (with a relative difference generally greater than or equal to 5 percent across trials).
Ø indicates a null effect (with a relative difference generally less than 5 percent across trials).
↑↓ indicates inconsistent findings (some trials reported improvement with meditation [relative to control] while others showed no improvement or improvement in the control group [relative to meditation]).
Magnitude based on relative difference in the change score: This is a relative percent difference, using the baseline mean in the meditation group as the denominator. For example, if the meditation group improves from a 10 to 19 on a mental health scale and the control group improves from 11 to 16 on the same scale, the relative difference between groups in the change score is: (((19-10)-(16-11))/10)x100=40%. The interpretation is that there is a 40% relative improvement on the mental health scale in the meditation group compared with the control group. Improvement in all scales is indicated in the positive direction. A positive relative percent difference means that the score improved more in the intervention group than in the control group
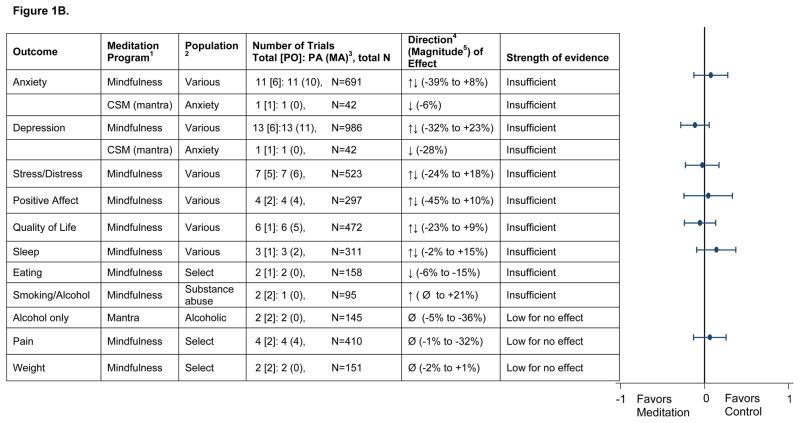
CSM = Clinically Standardized Meditation, a mantra meditation program; TM=Transcendental Meditation, a mantra meditation program
CHF = Congestive Heart Failure; CAD = Coronary Artery Disease
PO = Number of trials in which this was a primary outcome for the trial; PA = Primary Analysis; MA = Meta-analysis; N = sample size
Direction based on relative difference in change analysis:
↑ indicates that the meditation group improved relative to the control group (with a relative difference generally greater than or equal to 5 percent across trials).
↓ indicates the meditation group worsened relative to the control group (with a relative difference generally greater than or equal to 5 percent across trials).
Ø indicates a null effect (with a relative difference generally less than 5 percent across trials).
↑↓ indicates inconsistent findings (some trials reported improvement with meditation [relative to control] while others showed no improvement or improvement in the control group [relative to meditation]).
Magnitude based on relative difference in the change score: This is a relative percent difference, using the baseline mean in the meditation group as the denominator. For example, if the meditation group improves from a 10 to 19 on a mental health scale and the control group improves from 11 to 16 on the same scale, the relative difference between groups in the change score is: (((19-10)-(16-11))/10)x100=40%. The interpretation is that there is a 40% relative improvement on the mental health scale in the meditation group compared with the control group. Improvement in all scales is indicated in the positive direction. A positive relative percent difference means that the score improved more in the intervention group than in the control group
Comment in
-
Moving toward evidence-based complementary care.JAMA Intern Med. 2014 Mar;174(3):368-9. doi: 10.1001/jamainternmed.2013.12995. JAMA Intern Med. 2014. PMID: 24395188 No abstract available.
-
Meditation intervention reviews.JAMA Intern Med. 2014 Jul;174(7):1193. doi: 10.1001/jamainternmed.2014.1419. JAMA Intern Med. 2014. PMID: 25003876 No abstract available.
-
Meditation intervention reviews.JAMA Intern Med. 2014 Jul;174(7):1193-4. doi: 10.1001/jamainternmed.2014.1422. JAMA Intern Med. 2014. PMID: 25003877 No abstract available.
-
Meditation intervention reviews.JAMA Intern Med. 2014 Jul;174(7):1194-5. doi: 10.1001/jamainternmed.2014.1924. JAMA Intern Med. 2014. PMID: 25003878 Free PMC article. No abstract available.
-
Meditation intervention reviews--reply.JAMA Intern Med. 2014 Jul;174(7):1195. doi: 10.1001/jamainternmed.2014.1393. JAMA Intern Med. 2014. PMID: 25003880 No abstract available.
References
-
- Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States, 2007. Natl Health Stat Report. 2008;(12):1–23. - PubMed
-
- Rapgay L, Bystrisky A. Classical mindfulness: an introduction to its theory and practice for clinical application. Ann N Y Acad Sci. 2009;1172:148–62. - PubMed
-
- Travis F, Shear J. Focused attention, open monitoring and automatic self-transcending: Categories to organize meditations from Vedic, Buddhist and Chinese traditions. Conscious Cogn. 2010 Dec;19(4):1110–8. - PubMed
-
- Chiesa A, Malinowski P. Mindfulness-based approaches: are they all the same? J Clin Psychol. 2011;67 (4):404–24. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
