

Inflammasome-independent IL-1β mediates autoinflammatory disease in Pstpip2-deficient mice
- PMID: 24395802
- PMCID: PMC3903222
- DOI: 10.1073/pnas.1318685111
Inflammasome-independent IL-1β mediates autoinflammatory disease in Pstpip2-deficient mice
Abstract
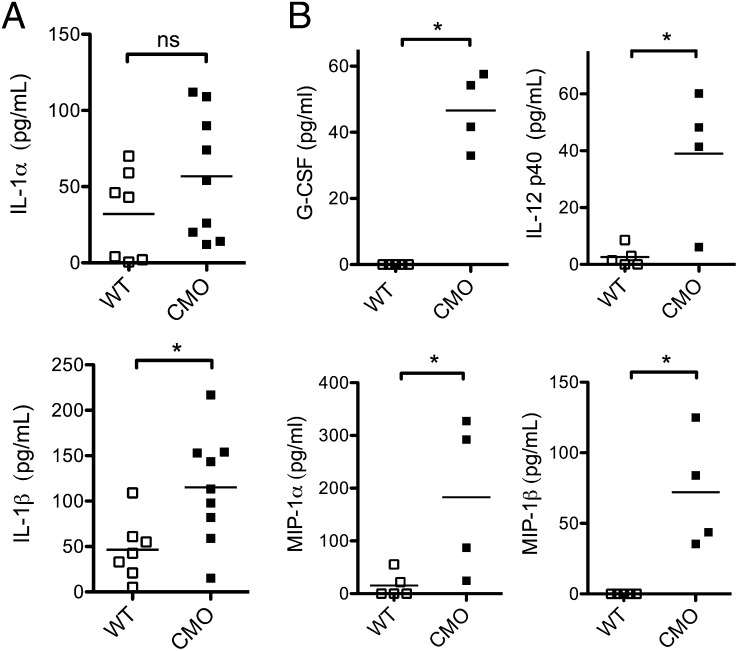
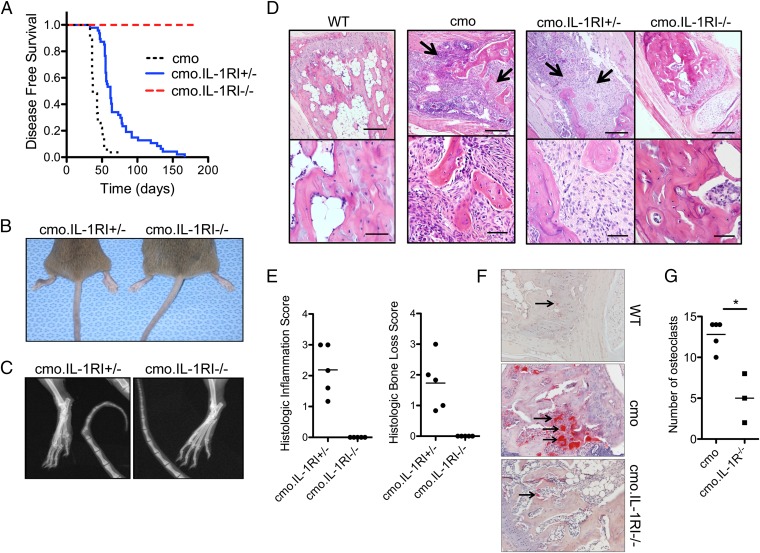
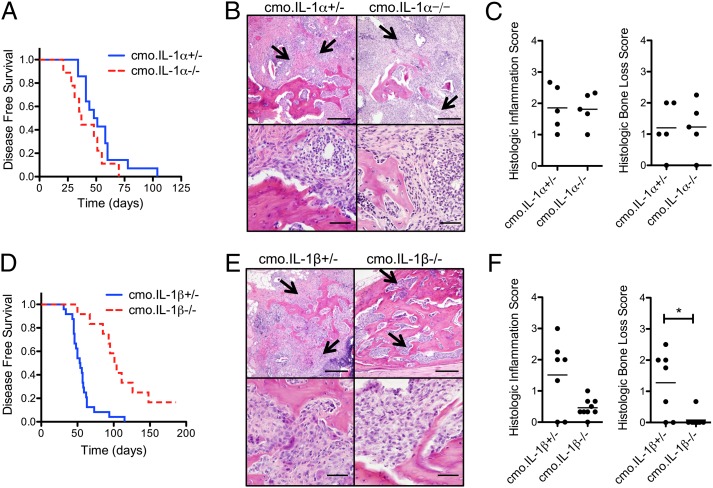
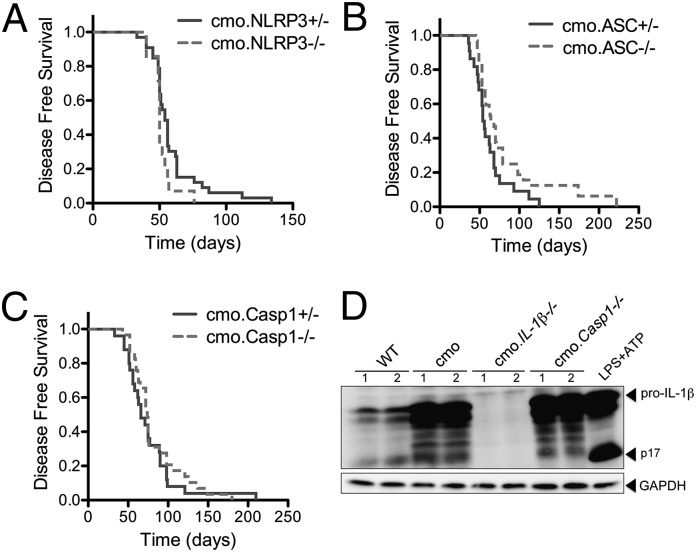
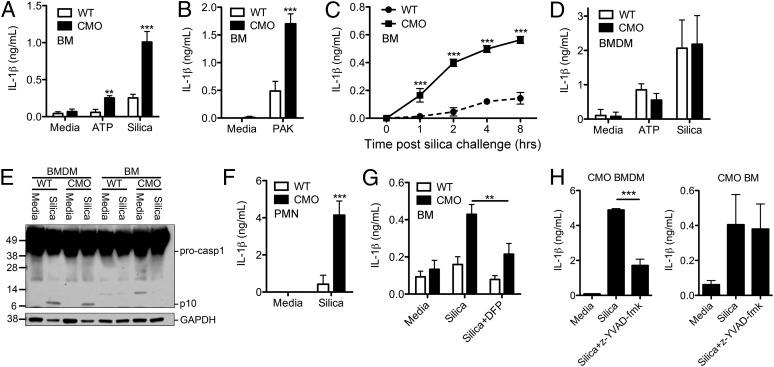
Chronic recurrent multifocal osteomyelitis (CRMO) is a human autoinflammatory disorder that primarily affects bone. Missense mutation (L98P) of proline-serine-threonine phosphatase-interacting protein 2 (Pstpip2) in mice leads to a disease that is phenotypically similar to CRMO called chronic multifocal osteomyelitis (cmo). Here we show that deficiency of IL-1RI in cmo mice resulted in a significant reduction in the time to onset of disease as well as the degree of bone pathology. Additionally, the proinflammatory cytokine IL-1β, but not IL-1α, played a critical role in the pathology observed in cmo mice. In contrast, disease in cmo mice was found to be independent of the nucleotide-binding domain, leucine-rich repeat-containing family, pyrin domain-containing 3 (NLRP3) inflammasome as well as caspase-1. Neutrophils, but not bone marrow-derived macrophages, from cmo mice secreted increased IL-1β in response to ATP, silica, and Pseudomonas aeruginosa compared with neutrophils from WT mice. This aberrant neutrophil response was sensitive to inhibition by serine protease inhibitors. These results demonstrate an inflammasome-independent role for IL-1β in disease progression of cmo and implicate neutrophils and neutrophil serine proteases in disease pathogenesis. These data provide a rationale for directly targeting IL-1RI or IL-1β as a therapeutic strategy in CRMO.
Keywords: chronic osteomyelitis; innate immunity.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Ferguson PJ, El-Shanti HI. Autoinflammatory bone disorders. Curr Opin Rheumatol. 2007;19(5):492–498. - PubMed
-
- Majeed HA, Al-Tarawna M, El-Shanti H, Kamel B, Al-Khalaileh F. The syndrome of chronic recurrent multifocal osteomyelitis and congenital dyserythropoietic anaemia. Report of a new family and a review. Eur J Pediatr. 2001;160(12):705–710. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
