

Early-onset neonatal sepsis
- PMID: 24396135
- PMCID: PMC3910904
- DOI: 10.1128/CMR.00031-13
Early-onset neonatal sepsis
Abstract
Early-onset sepsis remains a common and serious problem for neonates, especially preterm infants. Group B streptococcus (GBS) is the most common etiologic agent, while Escherichia coli is the most common cause of mortality. Current efforts toward maternal intrapartum antimicrobial prophylaxis have significantly reduced the rates of GBS disease but have been associated with increased rates of Gram-negative infections, especially among very-low-birth-weight infants. The diagnosis of neonatal sepsis is based on a combination of clinical presentation; the use of nonspecific markers, including C-reactive protein and procalcitonin (where available); blood cultures; and the use of molecular methods, including PCR. Cytokines, including interleukin 6 (IL-6), interleukin 8 (IL-8), gamma interferon (IFN-γ), and tumor necrosis factor alpha (TNF-α), and cell surface antigens, including soluble intercellular adhesion molecule (sICAM) and CD64, are also being increasingly examined for use as nonspecific screening measures for neonatal sepsis. Viruses, in particular enteroviruses, parechoviruses, and herpes simplex virus (HSV), should be considered in the differential diagnosis. Empirical treatment should be based on local patterns of antimicrobial resistance but typically consists of the use of ampicillin and gentamicin, or ampicillin and cefotaxime if meningitis is suspected, until the etiologic agent has been identified. Current research is focused primarily on development of vaccines against GBS.
Figures
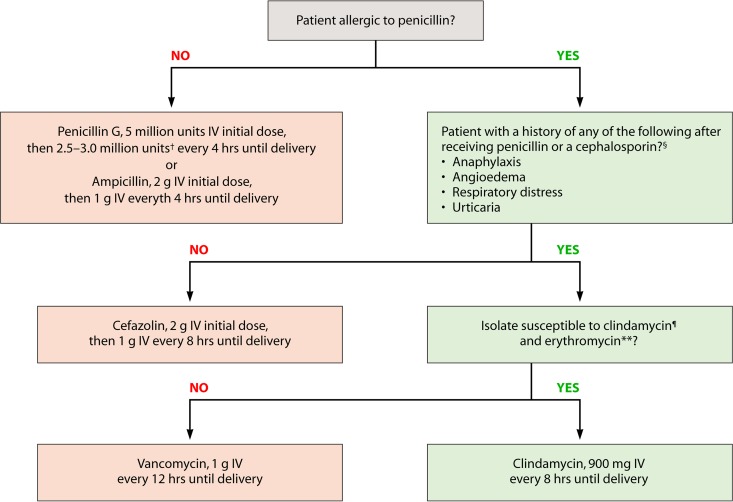
 , if laboratory facilities are adequate, clindamycin and erythromycin susceptibility testing should be performed on prenatal GBS isolates from penicillin-allergic women at high risk for anaphylaxis. If no susceptibility testing is performed or the results are not available at the time of labor, vancomycin is the preferred agent for GBS intrapartum prophylaxis for penicillin-allergic women at high risk for anaphylaxis. **, resistance to erythromycin is often but not always associated with clindamycin resistance. If an isolate is resistant to erythromycin, it might have inducible resistance to clindamycin, even if it appears susceptible to clindamycin. If a GBS isolate is susceptible to clindamycin and resistant to erythromycin and testing for inducible clindamycin resistance has been performed and is negative (no inducible resistance), then clindamycin can be used for GBS intrapartum prophylaxis instead of vancomycin. (Adapted from reference .)
, if laboratory facilities are adequate, clindamycin and erythromycin susceptibility testing should be performed on prenatal GBS isolates from penicillin-allergic women at high risk for anaphylaxis. If no susceptibility testing is performed or the results are not available at the time of labor, vancomycin is the preferred agent for GBS intrapartum prophylaxis for penicillin-allergic women at high risk for anaphylaxis. **, resistance to erythromycin is often but not always associated with clindamycin resistance. If an isolate is resistant to erythromycin, it might have inducible resistance to clindamycin, even if it appears susceptible to clindamycin. If a GBS isolate is susceptible to clindamycin and resistant to erythromycin and testing for inducible clindamycin resistance has been performed and is negative (no inducible resistance), then clindamycin can be used for GBS intrapartum prophylaxis instead of vancomycin. (Adapted from reference .)



References
-
- Edwards MS, Baker CJ. 2004. Sepsis in the newborn, p 545–561 In Gershon AA, Hotez PJ, Katz SL. (ed), Krugman's infectious diseases of children, 11th ed. Mosby, Philadelphia, PA
-
- Hornik CP, Fort P, Clark RH, Watt K, Benjamin DK, Jr, Smith PB, Manzoni P, Jacqz-Aigrain E, Kaguelidou F, Cohen-Wolkowiez M. 2012. Early and late onset sepsis in very-low-birth-weight infants from a large group of neonatal intensive care units. Early Hum. Dev. 88:S69–S74. 10.1016/S0378-3782(12)70019-1 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
