

The endemic treponematoses
- PMID: 24396138
- PMCID: PMC3910905
- DOI: 10.1128/CMR.00070-13
The endemic treponematoses
Abstract
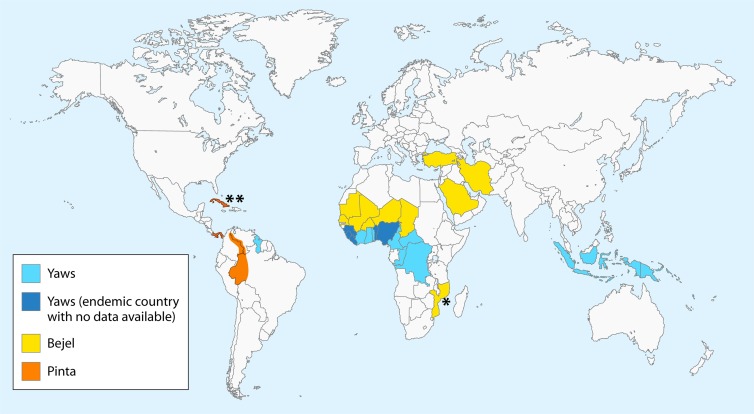
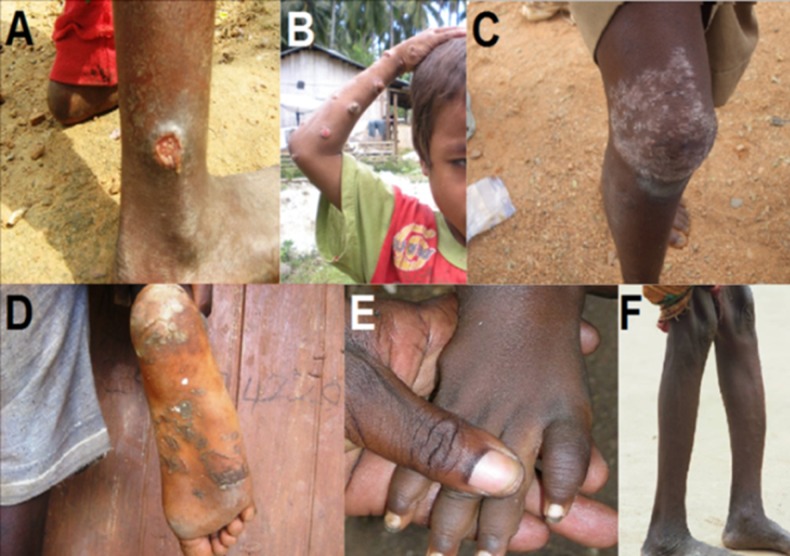
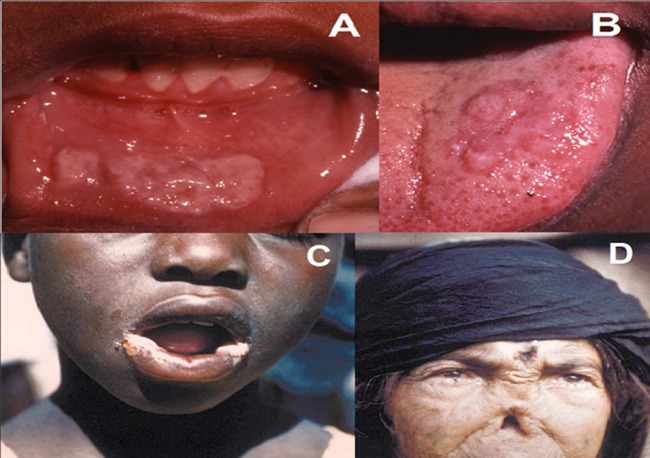
The agents of human treponematoses include four closely related members of the genus Treponema: three subspecies of Treponema pallidum plus Treponema carateum. T. pallidum subsp. pallidum causes venereal syphilis, while T. pallidum subsp. pertenue, T. pallidum subsp. endemicum, and T. carateum are the agents of the endemic treponematoses yaws, bejel (or endemic syphilis), and pinta, respectively. All human treponematoses share remarkable similarities in pathogenesis and clinical manifestations, consistent with the high genetic and antigenic relatedness of their etiological agents. Distinctive features have been identified in terms of age of acquisition, most common mode of transmission, and capacity for invasion of the central nervous system and fetus, although the accuracy of these purported differences is debated among investigators and no biological basis for these differences has been identified to date. In 2012, the World Health Organization (WHO) officially set a goal for yaws eradication by 2020. This challenging but potentially feasible endeavor is favored by the adoption of oral azithromycin for mass treatment and the currently focused distribution of yaws and endemic treponematoses and has revived global interest in these fascinating diseases and their causative agents.
Figures



References
-
- Paster BJ. 2010. Phylum XV. Spirochaetes Garrity and Holt 2001, p 471–566 In Krieg NR, Ludwig W, Whitman WB, Hedlund BP, Paster BJ, Staley JT, Ward N, Brown D, Parte A. (ed), Bergey's manual of systematic bacteriology. Springer, New York, NY
-
- Magnuson HJ, Eagle H, Fleischman R. 1948. The minimal infectious inoculum of Spirochaeta pallida (Nichols Strain), and a consideration of its rate of multiplication in vivo. Am. J. Syphilis 32:1–18 - PubMed
-
- Turner TB, Hollander DH. 1957. Biology of the treponematoses. World Health Organization, Geneva, Switzerland - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
