

Application of Queuing Analytic Theory to Decrease Waiting Times in Emergency Department: Does it Make Sense?
- PMID: 24396756
- PMCID: PMC3876544
- DOI: 10.5812/atr.7177
Application of Queuing Analytic Theory to Decrease Waiting Times in Emergency Department: Does it Make Sense?
Abstract
Background: Patients who receive care in an emergency department (ED), are usually unattended while waiting in queues.
Objectives: This study was done to determine, whether the application of queuing theory analysis might shorten the waiting times of patients admitted to emergency wards.
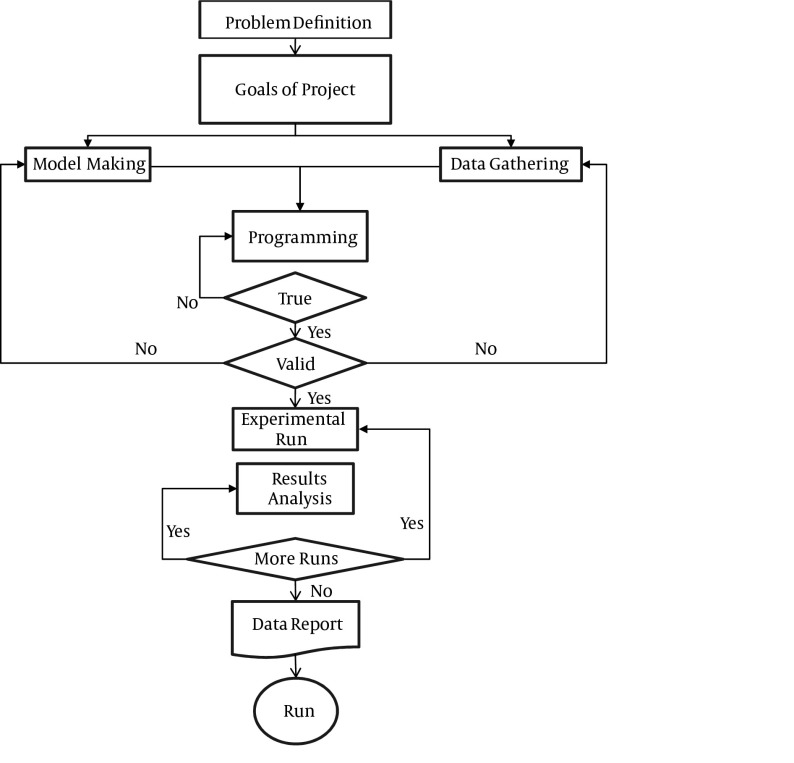
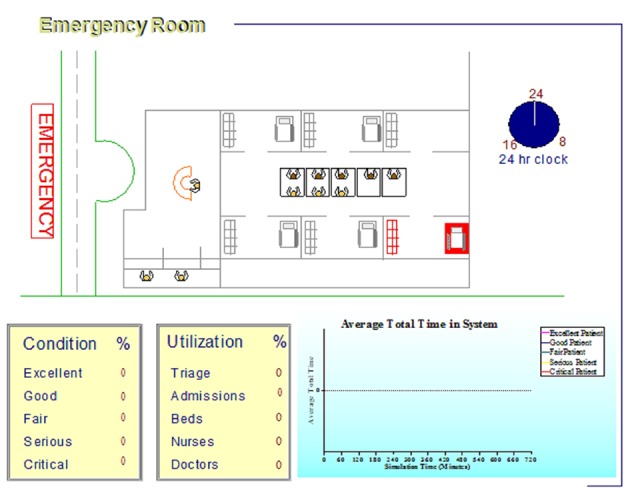
Patients and methods: This was an operational study to use queuing theory analysis in the ED. In the first phase, a field study was conducted to delineate the performance of the ED and enter the data obtained into simulator software. In the second phase, "ARENA" software was used for modeling, analysis, creating a simulation and improving the movement of patients in the ED. Validity of the model was confirmed through comparison of the results with the real data using the same instrument. The third phase of the study concerned modeling in order to assess the effect of various operational strategies, on the queue waiting time of patients who were receiving care in the ED.
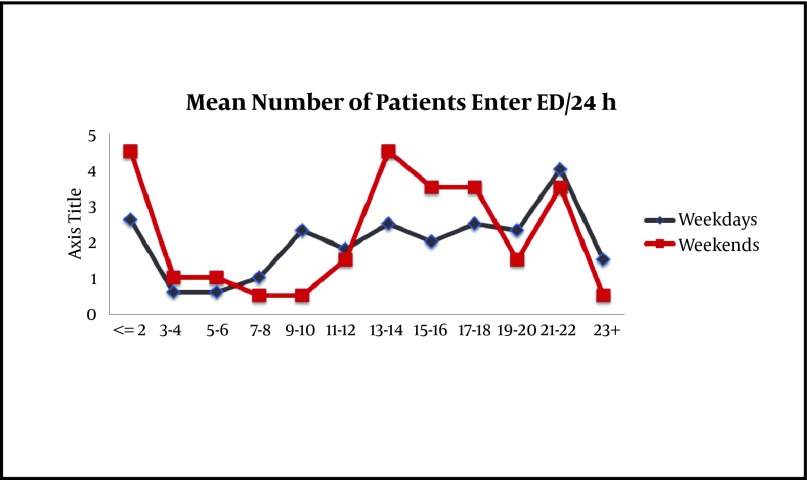
Results: In the first phase, it was shown that 47.7% of the 3000 patient records were cases referred for trauma treatment, and the remaining 52.3% were referred for non-trauma services. A total of 56% of the cases were male and 44% female. Maximum input was 4.5 patients per hour and the minimum input was 0.5 per hour. The average length of stay for patients in the trauma section was three hours, while for the non-trauma section it was four hours. In the second phase, modeling was tested with common scenarios. In the third phase, the scenario with the addition of one or more senior emergency resident(s) on each shift resulted in a decreased length of stay from 4 to 3.75 hours. Moreover, the addition of one bed to the Intensive Care Unit (ICU) and/or Critical Care Unit (CCU) in the study hospital, reduced the occupancy rate of the nursing service from 76% to 67%. By adding another clerk to take electrocardiograms (ECG) in the ED, the average time from a request to performing the procedure is reduced from 26 to 18 minutes. Furthermore, the addition of 50% more staff to the laboratory and specialist consultations led to a 90 minute reduction in the length of stay. It was also shown that earlier consultations had no effect on the length of stay.
Conclusions: Application of queuing theory analysis can improve movement and reduce the waiting times of patients in bottlenecks within the ED throughput.
Keywords: Emergency Department; Operational Research; Quality Improvement; Queuing.
Figures
References
-
- Brandeau ML, Sainfort F, Pierskalla WP. Operations research and health care: a handbook of methods and applications. Library of Congress; 2004.
-
- Salustri L, Sbandi P, Brailsford S, Brocato R. Modeling and simulating the process of an accident and emergency department. Proceedings of the 38th conference on Winter simulation; Monterey, California: Winter Simulation Conference; 2006. pp. 446–52.
-
- Komashie A, Mousavi A. Modeling Emergency Departments Using Descrete EventSimulation Techniques. proceedings of the 2005 winter simulation conference; Orlando, FL, USA.: 2005.
-
- Preston K, White J. A survey of data resources for simulating patient flows in healthcare delivery systems. Proceedings of the 37th conference on Winter simulation; Orlando, Florida: Winter Simulation Conference; 2005. pp. 926–35.
LinkOut - more resources
Full Text Sources