

Modification of elastic stable intramedullary nailing with a 3rd nail in a femoral spiral fracture model - results of biomechanical testing and a prospective clinical study
- PMID: 24397612
- PMCID: PMC4029588
- DOI: 10.1186/1471-2474-15-3
Modification of elastic stable intramedullary nailing with a 3rd nail in a femoral spiral fracture model - results of biomechanical testing and a prospective clinical study
Abstract
Background: Elastic stable intramedullary nailing (ESIN) is the standard treatment for displaced diaphyseal femoral fractures in children. However, high complication rates (10-50%) are reported in complex fractures. This biomechanical study compares the stiffness with a 3rd nail implanted to that in the classical 2C-shaped configuration and presents the application into clinical practice.
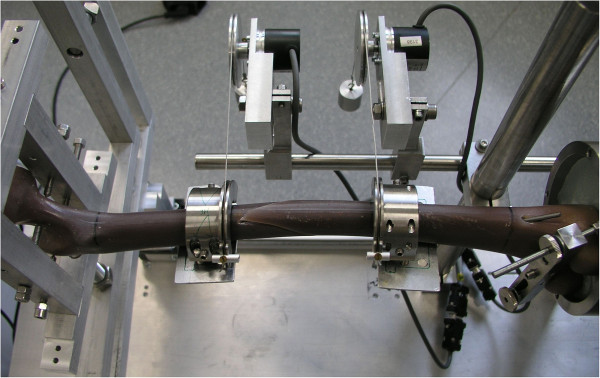
Methods: For each of the 3 configurations of ESIN-osteosynthesis with titanium nails eight composite femoral grafts (Sawbones®) with an identical spiral fracture were used: 2C configuration (2C-shaped nails, 2 × 3.5 mm), 3CM configuration (3rd nail from medial) and 3CL configuration (3rd nail from lateral). Each group underwent biomechanical testing in 4-point bending, internal/external rotation and axial compression.
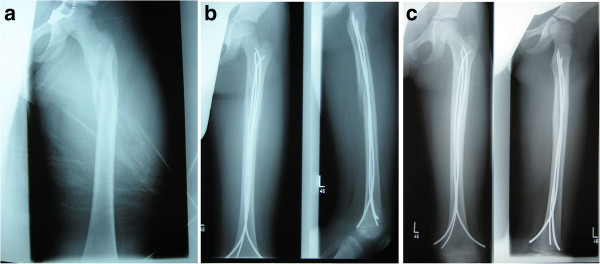
Results: 2C and 3CM configurations showed no significant differences in this spiroid type fracture model. 3CL had a significantly higher stiffness during anterior-posterior bending, internal rotation and 9° compression than 2C, and was stiffer in the lateral-medial direction than 3CM. The 3CL was less stable during p-a bending and external rotation than both the others. As biomechanical testing showed a higher stability for the 3CL configuration in two (a-p corresponding to recurvation and 9° compression to shortening) of three directions associated with the most important clinical problems, we added a 3rd nail in ESIN-osteosynthesis for femoral fractures. 11 boys and 6 girls (2.5-15 years) were treated with modified ESIN of whom 12 were '3CL'; due to the individual character of the fractures 4 patients were treated with '3CM' (third nail from medial) and as an exception 1 adolescent with 4 nails and one boy with plate osteosynthesis. No additional stabilizations or re-operations were necessary. All patients achieved full points in the Harris-Score at follow-up; no limb length discrepancy occurred.
Conclusion: The 3CL configuration provided a significantly higher stiffness than 2C and 3CM configurations in this biomechanical model. These results were successfully transmitted into clinical practice. All children, treated by 3CL or 3CM according to the individual character of each fracture, needed no additional stabilization and had no Re-Do operations. As a consequence, at our hospital all children with femoral diaphyseal fractures with open physis are treated with this modified ESIN-technique.
Trial registration: ClinicalTrials.gov NCT01673048.
Figures




Similar articles
-
Improving stability of elastic stable intramedullary nailing in a transverse midshaft femur fracture model: biomechanical analysis of using end caps or a third nail.J Orthop Surg Res. 2015 Jun 25;10:96. doi: 10.1186/s13018-015-0239-z. J Orthop Surg Res. 2015. PMID: 26109085 Free PMC article.
-
Additional Tension Screws Improve Stability in Elastic Stable Intramedullary Nailing: Biomechanical Analysis of a Femur Spiral Fracture Model.Eur J Pediatr Surg. 2015 Aug;25(4):365-72. doi: 10.1055/s-0034-1376394. Epub 2014 Jun 10. Eur J Pediatr Surg. 2015. PMID: 24914565
-
Biomechanical analysis of a synthetic femoral spiral fracture model: Do end caps improve retrograde flexible intramedullary nail fixation?J Orthop Surg Res. 2011 Sep 18;6:46. doi: 10.1186/1749-799X-6-46. J Orthop Surg Res. 2011. PMID: 21923948 Free PMC article.
-
Treatment of pediatric femoral shaft fractures with elastic stable intramedullary nails versus external fixation: A meta-analysis.Orthop Traumatol Surg Res. 2020 Nov;106(7):1305-1311. doi: 10.1016/j.otsr.2020.06.012. Epub 2020 Oct 17. Orthop Traumatol Surg Res. 2020. PMID: 33082120
-
A meta-analysis of external fixation and flexible intramedullary nails for femoral fractures in children.Acta Orthop Belg. 2016 Dec;82(4):673-680. Acta Orthop Belg. 2016. PMID: 29182105 Review.
Cited by
-
Closed reduction and intramedullary nails for acute completely displaced femoral diaphysis fracture in children aged 2-6.Front Pediatr. 2024 Apr 11;12:1346456. doi: 10.3389/fped.2024.1346456. eCollection 2024. Front Pediatr. 2024. PMID: 38665374 Free PMC article.
-
Improving stability of elastic stable intramedullary nailing in a transverse midshaft femur fracture model: biomechanical analysis of using end caps or a third nail.J Orthop Surg Res. 2015 Jun 25;10:96. doi: 10.1186/s13018-015-0239-z. J Orthop Surg Res. 2015. PMID: 26109085 Free PMC article.
-
Is elastic stable intramedullary nail a good choice for pathological fractures of the proximal femur due to simple bone cyst in pediatric population?Medicine (Baltimore). 2020 Sep 25;99(39):e22364. doi: 10.1097/MD.0000000000022364. Medicine (Baltimore). 2020. PMID: 32991454 Free PMC article.
-
The effect of canal fill on paediatric femur fractures treated with titanium elastic nails.J Child Orthop. 2018 Feb 1;12(1):15-19. doi: 10.1302/1863-2548.12.170083. J Child Orthop. 2018. PMID: 29456749 Free PMC article.
-
Leg length discrepancy after skeletal maturity in patients treated with elastic intramedullary nails after femoral shaft fractures in childhood.J Child Orthop. 2022 Aug;16(4):276-284. doi: 10.1177/18632521221106388. Epub 2022 Aug 2. J Child Orthop. 2022. PMID: 35992517 Free PMC article.
References
-
- Leitlinien AF. Deutsche Gesellschaft für Kinderchirurgie. 2008. http://www.awmf.org/leitlinien/detail/ll/006-016.html.
-
- Dietz HG, Joppich I, Marzi I, Parsch K, Schlickewei W, Schmittenbecher PP. [Treatment of femoral fractures in childhood. Consensus report of the 19th meeting of the child traumatology section of the DGU, Munich, 23–24 June 2000] Unfallchirurg. 2001;104(8):788–790. doi: 10.1007/s001130170082. - DOI - PubMed
-
- Dietz HG, Schmittenbecher PP, Illing P. Intramedulläre Osteosynthese im Wachstumsalter. München Wien Baltimore: Urban + Schwarzenberg; 1997.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
