

Epidemiology of musculoskeletal upper extremity ambulatory surgery in the United States
- PMID: 24397703
- PMCID: PMC3893587
- DOI: 10.1186/1471-2474-15-4
Epidemiology of musculoskeletal upper extremity ambulatory surgery in the United States
Abstract
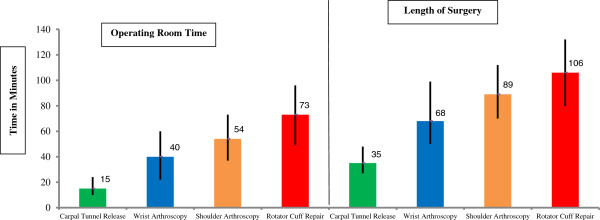
Background: Musculoskeletal disorders of the upper extremity are common reasons for patients to seek care and undergo ambulatory surgery. The objective of our study was to assess the overall and age-adjusted utilization rates of rotator cuff repair, shoulder arthroscopy performed for indications other than rotator cuff repair, carpal tunnel release, and wrist arthroscopy performed for indications other than carpal tunnel release in the United States. We also compared demographics, indications, and operating room time for these procedures.
Methods: We used the 2006 National Survey of Ambulatory Surgery to estimate the number of procedures of interest performed in the United States in 2006. We combined these data with population size estimates from the 2006 U.S. Census Bureau to calculate rates per 10,000 persons.
Results: An estimated 272,148 (95% confidence intervals (CI) = 218,994, 325,302) rotator cuff repairs, 257,541 (95% CI = 185,268, 329,814) shoulder arthroscopies excluding those for cuff repairs, 576,924 (95% CI = 459,239, 694,609) carpal tunnel releases, and 25,250 (95% CI = 17,304, 33,196) wrist arthroscopies excluding those for carpal tunnel release were performed. Overall, carpal tunnel release had the highest utilization rate (37.3 per 10,000 persons in persons of age 45-64 years; 38.7 per 10,000 persons in 65-74 year olds, and; 44.2 per 10,000 persons in the age-group 75 years and older). Among those undergoing rotator cuff repairs, those in the age-group 65-74 had the highest utilization (28.3 per 10,000 persons). The most common indications for non-cuff repair related shoulder arthroscopy were impingement syndrome, periarthritis, bursitis, and instability/SLAP tears. Non-carpal tunnel release related wrist arthroscopy was most commonly performed for ligament sprains and diagnostic arthroscopies for pain and articular cartilage disorders.
Conclusions: Our data shows substantial age and demographic differences in the utilization of these commonly performed upper extremity ambulatory procedures. While over one million upper extremity procedures of interest were performed, evidence-based clinical indications for these procedures remain poorly defined.
Figures
References
-
- Turkelson CM, Zhao G. Musculoskeletal conditions and disorders: occurence and healthcare use in the United States. Rosemont, IL: Department of Research and Scientific Affairs, American Academy of Orthopaedic Surgeons; 2009. http://www.aaos.org/research/stats/patientstats.asp.
-
- Hall MJ, Lawrence L. Ambulatory surgery in the United States. Adv Data . 1996;1998(300):1–16. - PubMed
-
- Lumsdon K, Anderson HJ, Burke M. New surgical technologies reshape hospital strategies. Hospitals. 1992;66(9):30–6, 38–40–2. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
