

Stage 0 osteonecrosis of the jaw in a patient on denosumab
- PMID: 24397946
- PMCID: PMC4045108
- DOI: 10.1016/j.joms.2013.09.008
Stage 0 osteonecrosis of the jaw in a patient on denosumab
Abstract
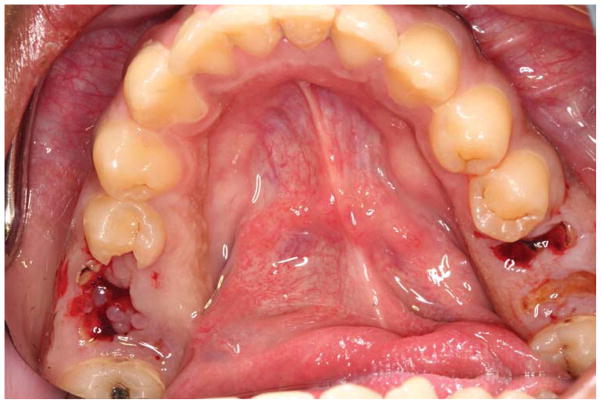
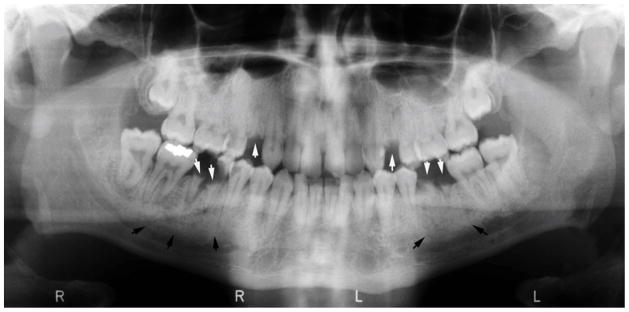
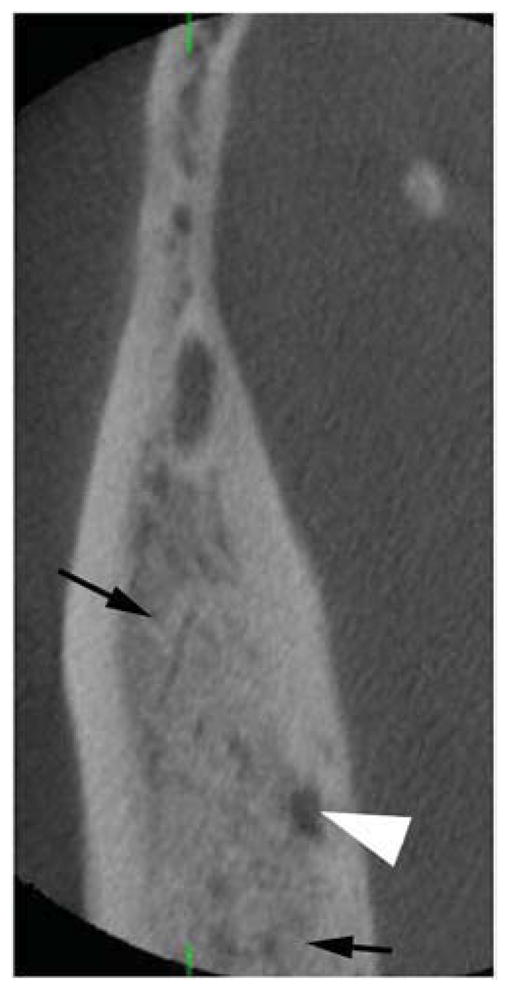
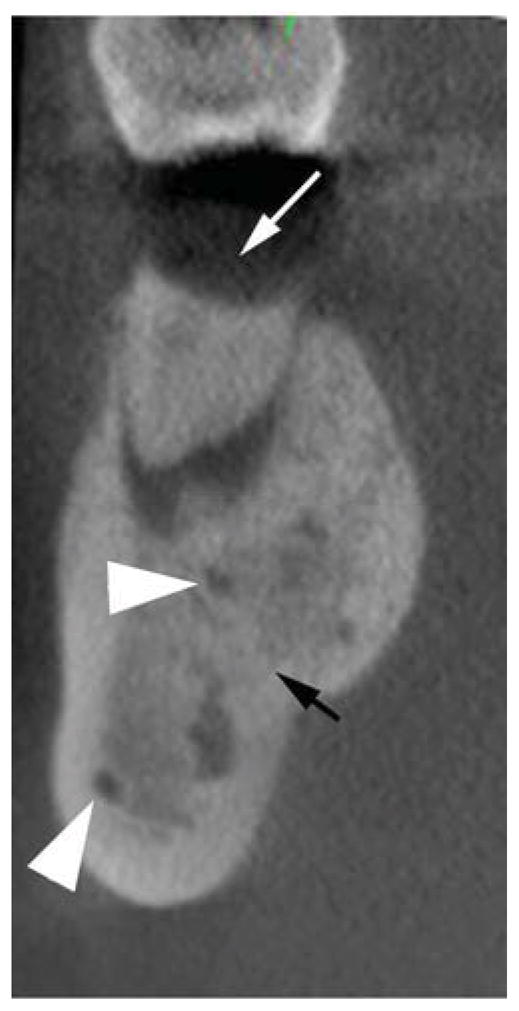
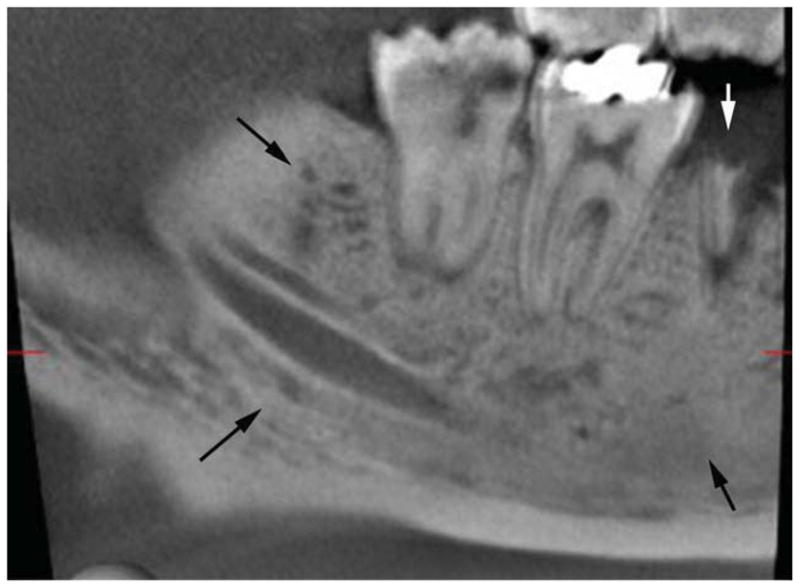
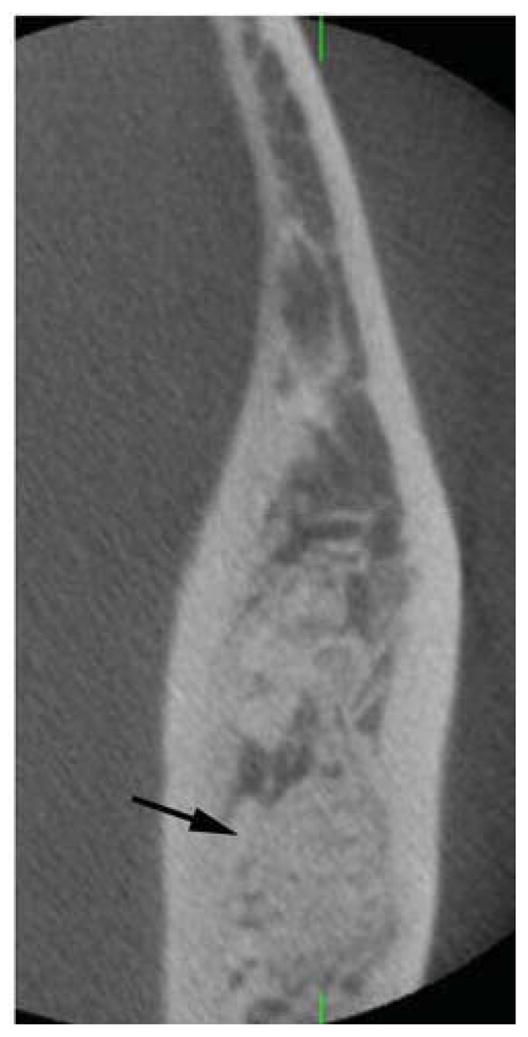
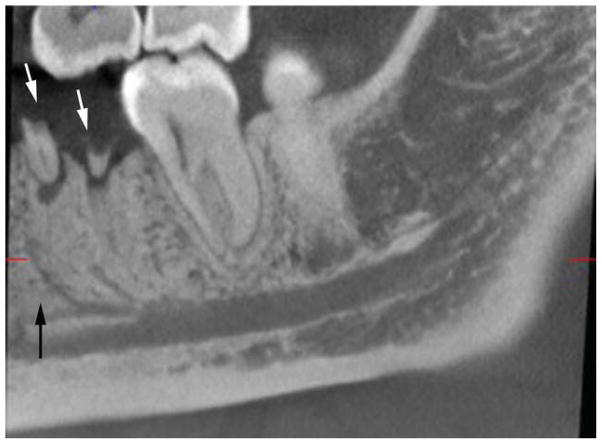
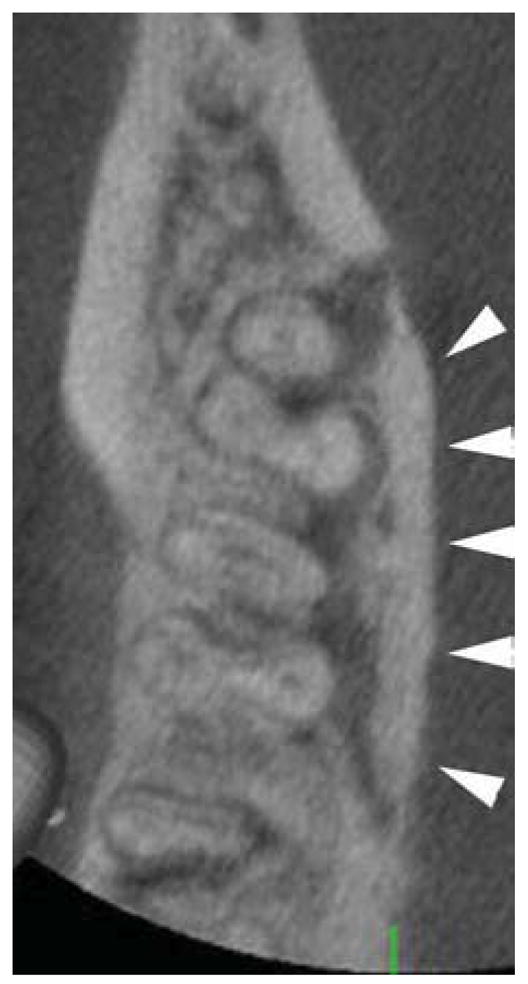
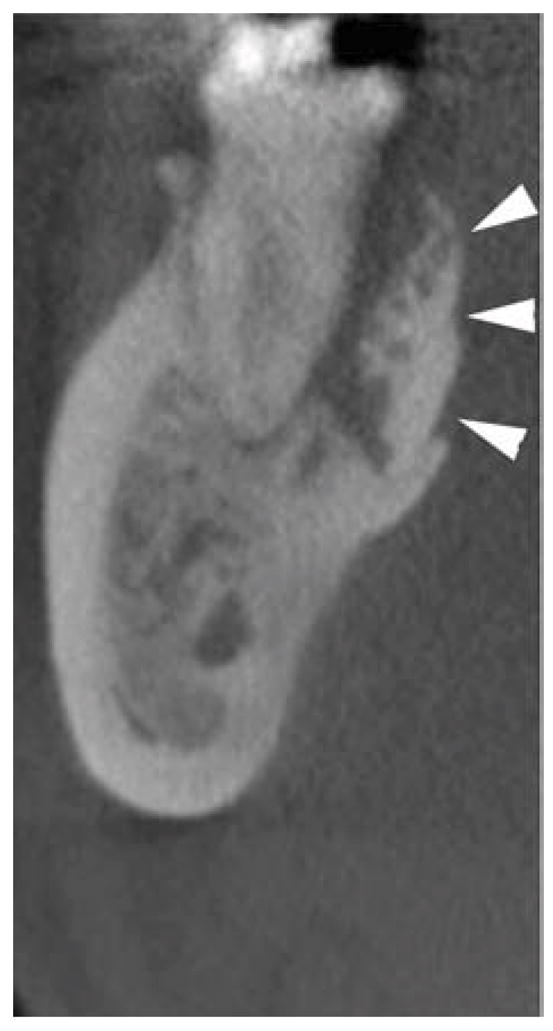
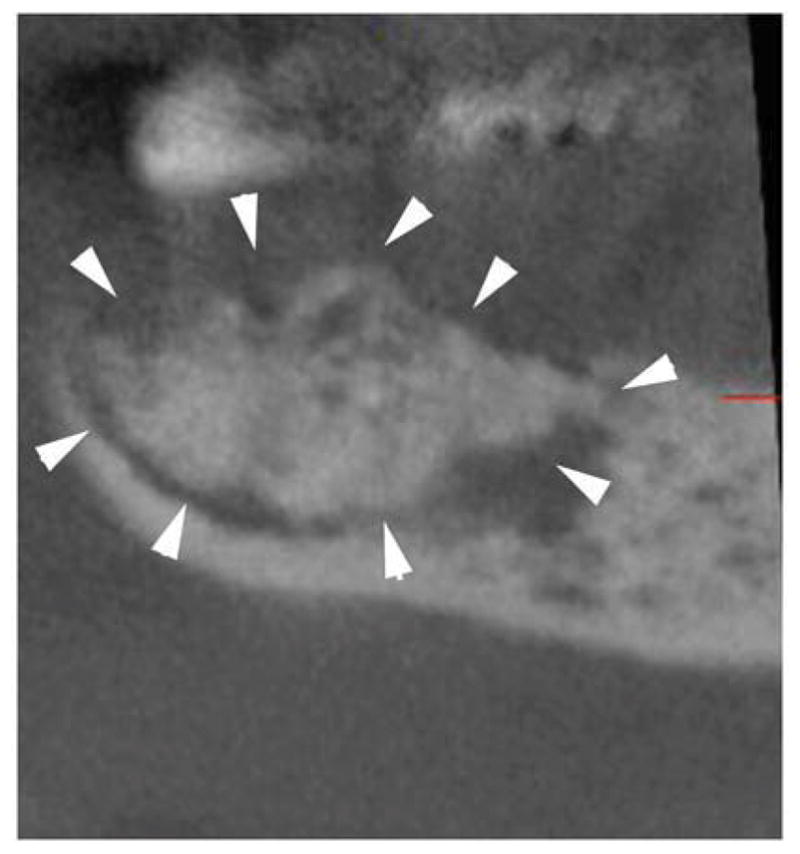
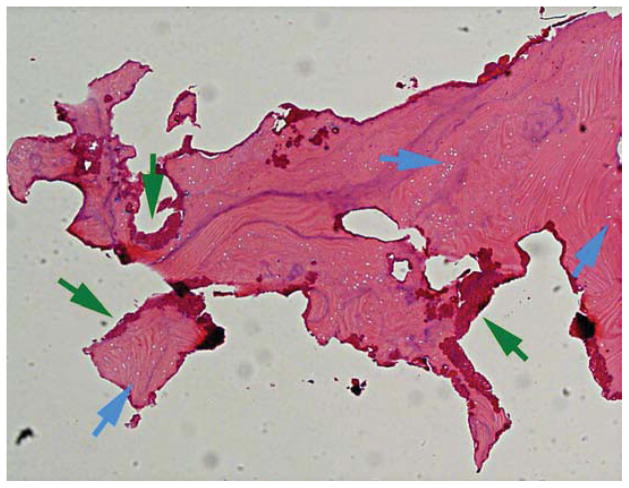
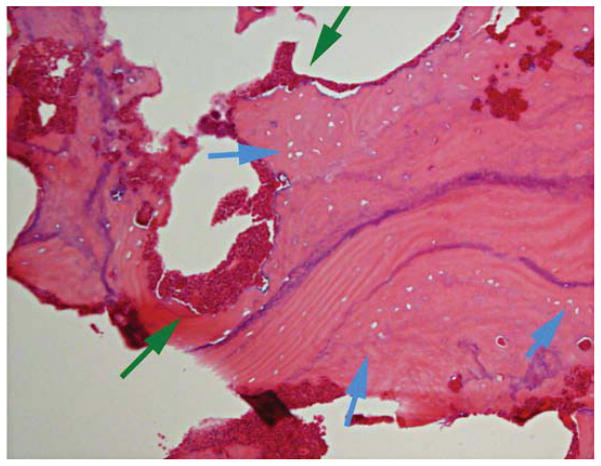
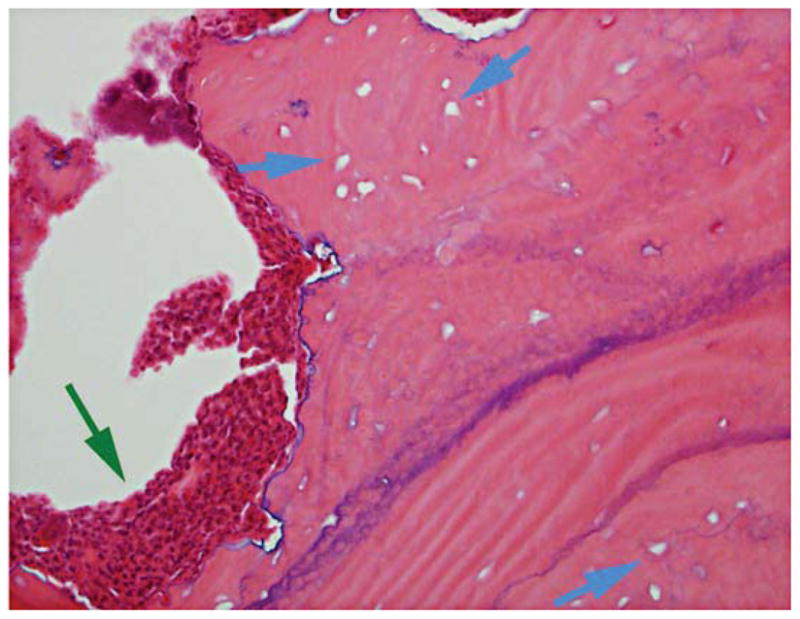
Osteonecrosis of the jaws (ONJ) is a complex disease involving multiple tissue and cell-type responses to wound healing or infection. AAOMS defines bisphosphonate related ONJ (BRONJ) as exposed, necrotic bone in the maxillofacial region that has persisted for more than 8 weeks in a patient with current or previous antiresorptive treatment, without a history of radiation therapy to the jaws. Since the first reported ONJ cases in 2003 and 2004, there has been little advancement in understanding the etiology and pathophysiology of ONJ. Many hypotheses have been proposed, including bisphosphonate (BP) toxicity to oral epithelium, altered wound healing after tooth extraction, high turnover of the mandible and maxilla, oral biofilm formation, infection and inflammation, and suppression of angiogenesis and bone turnover. The current classification system of ONJ involves stages 0 to 3 and is based on patient clinical presentation. This report describes a case of stage 0 ONJ in a patient on denosumab and indicates the full-spectrum similarities between BP- and denosumab-associated ONJ clinically, radiographically, and histologically.
Published by Elsevier Inc.
Figures



References
-
- Farah CS, Savage NW. Oral ulceration with bone sequestration. Aust Dent J. 2003;48:61. - PubMed
-
- Meer S, Coleman H, Altini M, Alexander T. Mandibular osteomyelitis and tooth exfoliation following zoster-CMV co-infection. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;101:70. - PubMed
-
- Schwartz HC. Osteonecrosis of the jaws: a complication of cancer chemotherapy. Head Neck Surg. 1982;4:251. - PubMed
-
- Advisory Task Force on Bisphosphonate-Related Ostenonecrosis of the Jaws AAoO, Maxillofacial S American Association of Oral and Maxillofacial Surgeons position paper on bisphosphonate-related osteonecrosis of the jaws. J Oral Maxillofac Surg. 2007;65:369. - PubMed
-
- Ruggiero SL, Dodson TB, Assael LA, Landesberg R, Marx RE, Mehrotra B American Association of O Maxillofacial S. American Association of Oral and Maxillofacial Surgeons position paper on bisphosphonate-related osteonecrosis of the jaws--2009 update. J Oral Maxillofac Surg. 2009;67:2. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
