

Bladeless direct optical trocar insertion in laparoscopic procedures on the obese patient
- PMID: 24398192
- PMCID: PMC3866054
- DOI: 10.4293/108680813X13693422519398
Bladeless direct optical trocar insertion in laparoscopic procedures on the obese patient
Abstract
Background: Recently, we have shown advantages of a direct optical entry (DOE) using a bladeless trocar in comparison with the open Hasson technique (OHT) in older reproductive-age women with previous operations, as well as in comparison with Veress needle entry in reproductive-age and postmenopausal women.
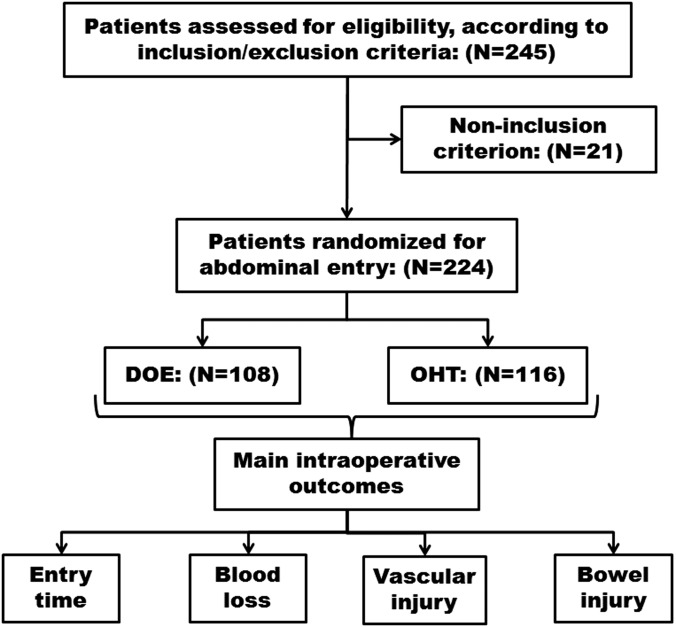
Objectives: A prospective multicenter randomized study to determine whether the DOE is feasible for establishing safe and rapid entry into the abdomen in comparison with those of the OHT in reproductive-age obese women.
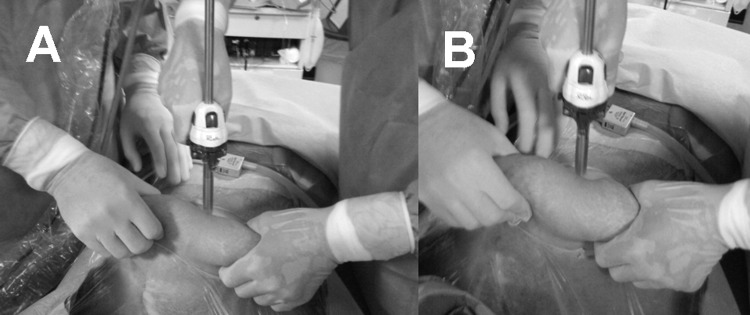
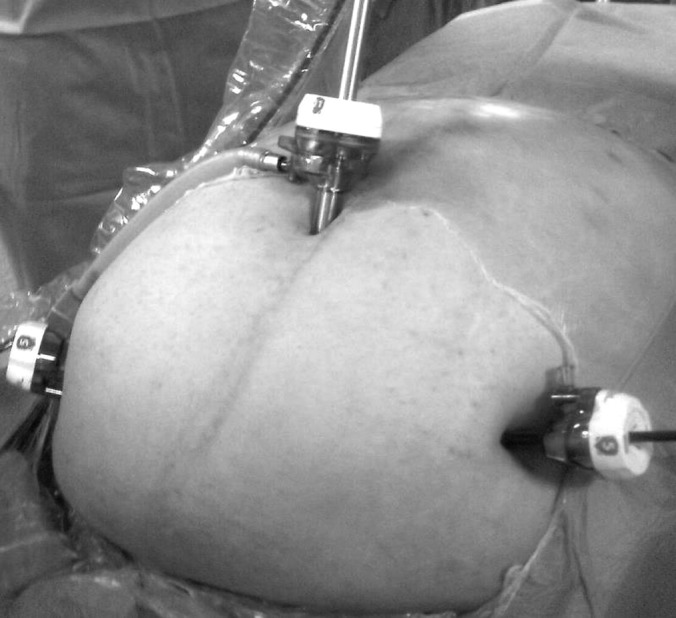
Methods: Two types of surgical techniques were blindly applied in 224 obese reproductive-age women with benign neoplastic diseases of ovary and uterus. Namely, laparoscopic entry into the abdomen in 108 patients was performed by DOE and in 116 women by OHT. Following parameters (entry time in seconds needed to establish the intra-abdominal vision after pneumoperitoneum, blood loss, occurrence of vascular and/or bowel injuries) were compared during surgery as main outcomes.
Results: Main baseline characteristics of patients, including age (36.1 ± 4.5 vs 35.7 ± 5.8), body mass index (34.9 ± 5.1 vs 35.1 ± 4.9 kg/m(2)), and parity (2.1 ± 0.4 vs 1.9 ± 0.9), were not significantly different between the DOE and OHT groups (P > .05). While intraoperative parameters such as the entry time (71.9 ± 3.7 vs 215.1 ± 6.2 seconds) and blood loss value (9.7 ± 6.1 vs 12.2 ± 2.9 mL) were significantly reduced in the DOE group in comparison with those of OHT group (respectively, P < .0001 and < .01), there were also trends to slight decrease of the occurrence of the minor injuries, manifested as omental small vessels rupture (0 of 108 vs 4 of 116) and punctures and pinches of jejunal serosa (0 of 108 vs 3 of 116) in patients of the DOE group in comparison with those of OHT group (respectively, P = .0515 and = .0925).
Conclusions: DOE reduced entry time and blood loss with trends to slightly decrease of the occurrence of the minor vascular and bowel injuries, thus enabling a possible alternative to OHT in obese women; however, further larger trials need to confirm the possible additional benefits of a DOE.
Figures

References
-
- Tinelli A, Malvasi A, Schneider AJ, et al. First abdominal access in gynecological laparoscopy: which method to utilize? [in Italian]. Minerva Ginecol. 2006;58(5):429–440 - PubMed
-
- Tinelli A. Laparoscopic Entry: Traditional Methods, New Insights and Novel Approaches. London, UK: Springer, 2012
-
- Ahmad G, O'Flynn H, Duffy JM, Phillips K, Watson A. Laparoscopic entry techniques. Cochrane Database Syst Rev. 2012;2:CD006583. - PubMed
-
- Ambardar S, Cabot J, Cekic V, et al. Abdominal wall dimensions and umbilical position vary widely with BMI and should be taken into account when choosing port locations. Surg Endosc. 2009;23(9):1995–2000 - PubMed
-
- Stany MP, Winter WE, 3rd, Dainty L, Lockrow E, Carlson JW. Laparoscopic exposure in obese high-risk patients with mechanical displacement of the abdominal wall. Obstet Gynecol. 2004;103(2):383–386 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical