

Automated near-real-time clinical performance feedback for anesthesiology residents: one piece of the milestones puzzle
- PMID: 24398735
- PMCID: PMC3893706
- DOI: 10.1097/ALN.0000000000000071
Automated near-real-time clinical performance feedback for anesthesiology residents: one piece of the milestones puzzle
Abstract
Background: Anesthesiology residencies are developing trainee assessment tools to evaluate 25 milestones that map to the six core competencies. The effort will be facilitated by development of automated methods to capture, assess, and report trainee performance to program directors, the Accreditation Council for Graduate Medical Education and the trainees themselves.
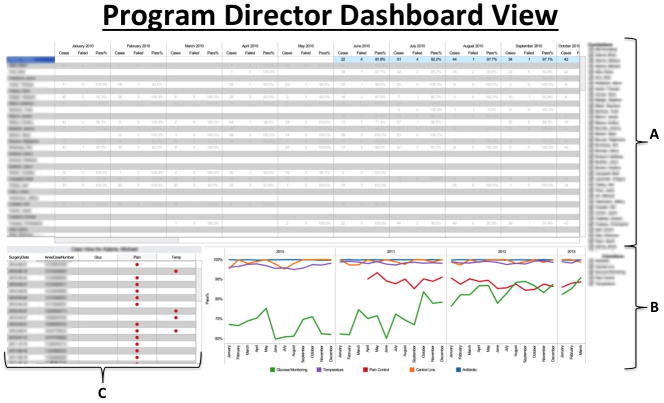
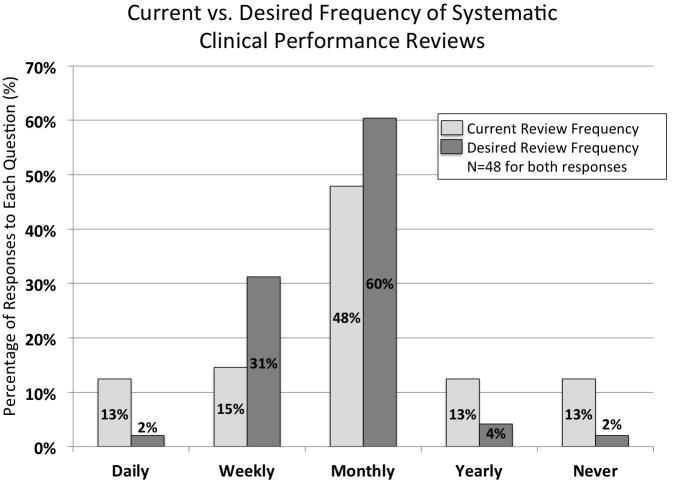
Methods: The authors leveraged a perioperative information management system to develop an automated, near-real-time performance capture and feedback tool that provides objective data on clinical performance and requires minimal administrative effort. Before development, the authors surveyed trainees about satisfaction with clinical performance feedback and about preferences for future feedback.
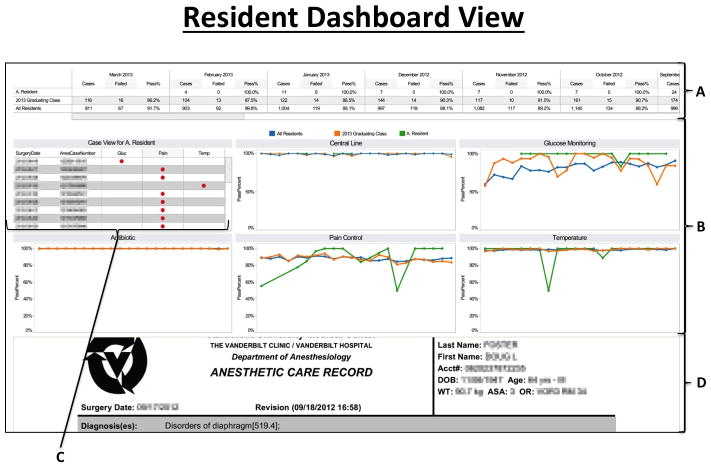
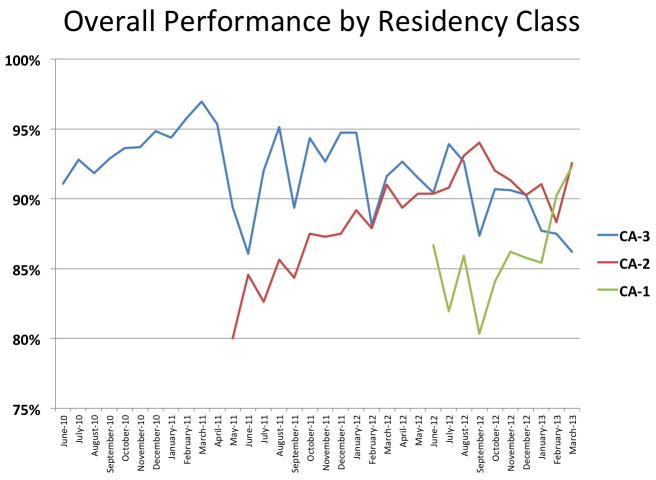
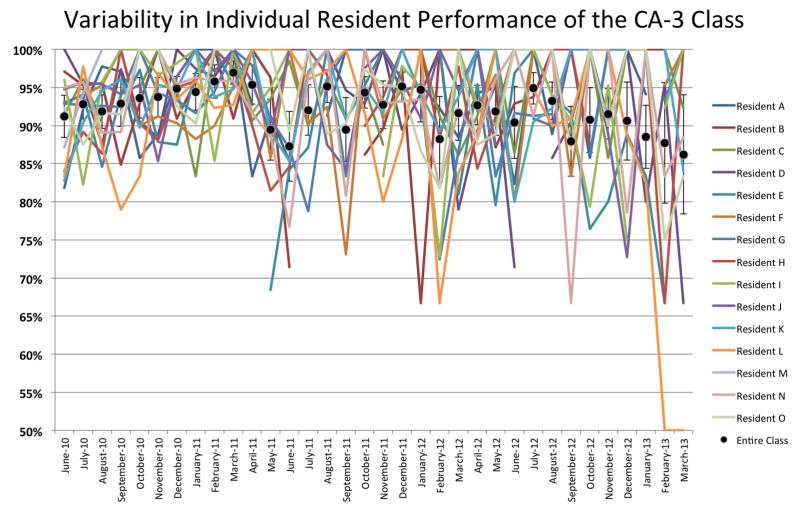
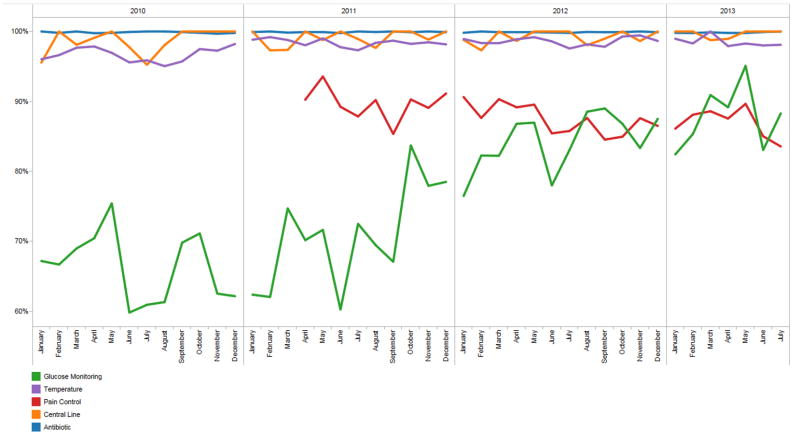
Results: Resident performance on 24,154 completed cases has been incorporated into the authors' automated dashboard, and trainees now have access to their own performance data. Eighty percent (48 of 60) of the residents responded to the feedback survey. Overall, residents "agreed/strongly agreed" that they desire frequent updates on their clinical performance on defined quality metrics and that they desired to see how they compared with the residency as a whole. Before deployment of the new tool, they "disagreed" that they were receiving feedback in a timely manner. Survey results were used to guide the format of the feedback tool that has been implemented.
Conclusion: The authors demonstrate the implementation of a system that provides near-real-time feedback concerning resident performance on an extensible series of quality metrics, and which is responsive to requests arising from resident feedback about desired reporting mechanisms.
Conflict of interest statement
Figures
References
-
- Nasca TJ, Philibert I, Brigham T, Flynn TC. The next GME accreditation system--rationale and benefits. N Engl J Med. 2012;366:1051–6. - PubMed
-
- Brown DL. Using an anesthesia information management system to improve case log data entry and resident workflow. Anesth Analg. 2011;112:260–1. - PubMed
-
- Simpao A, Heitz JW, McNulty SE, Chekemian B, Brenn BR, Epstein RH. The design and implementation of an automated system for logging clinical experiences using an anesthesia information management system. Anesth Analg. 2011;112:422–9. - PubMed
-
- O’Reilly M, Talsma A, VanRiper S, Kheterpal S, Burney R. An anesthesia information system designed to provide physician-specific feedback improves timely administration of prophylactic antibiotics. Anesth Analg. 2006;103:908–12. - PubMed
-
- Spring SF, Sandberg WS, Anupama S, Walsh JL, Driscoll WD, Raines DE. Automated documentation error detection and notification improves anesthesia billing performance. Anesthesiology. 2007;106:157–63. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
