

Predictors of neurocognitive outcomes on antiretroviral therapy after cryptococcal meningitis: a prospective cohort study
- PMID: 24399496
- PMCID: PMC4033836
- DOI: 10.1007/s11011-013-9476-1
Predictors of neurocognitive outcomes on antiretroviral therapy after cryptococcal meningitis: a prospective cohort study
Abstract
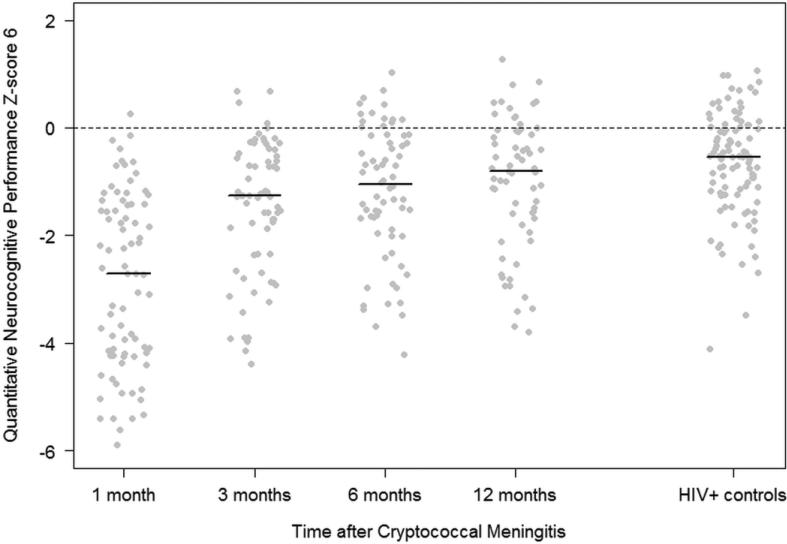
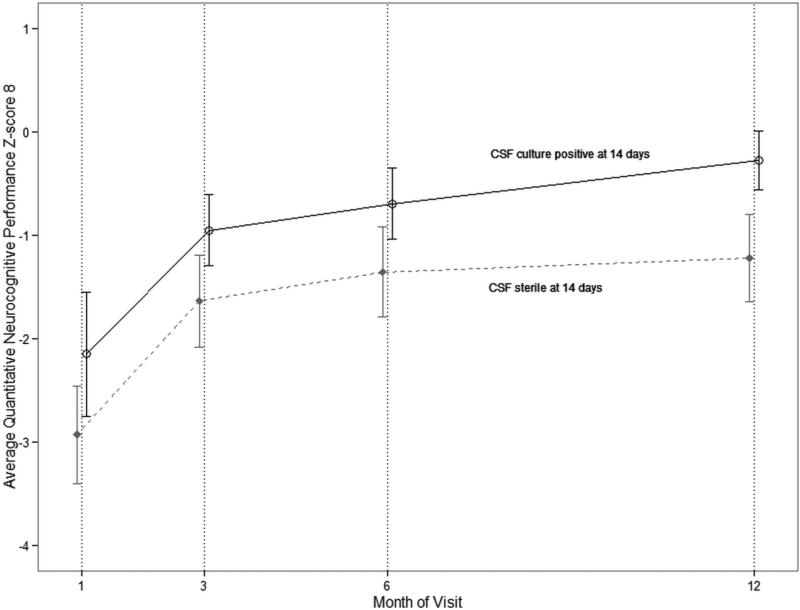
Cryptococcal meningitis is the most common cause of adult meningitis in Africa, yet neurocognitive outcomes are unknown. We investigated the incidence and predictors of neurologic impairment among cryptococcal survivors. HIV-infected, antiretroviral-naive Ugandans with cryptococcal meningitis underwent standardized neuropsychological testing at 1, 3, 6, and 12 months. A quantitative neurocognitive performance z-score (QNPZ) was calculated based on population z-scores from HIV-negative Ugandans (n = 100). Comparison was made with an HIV-infected, non-meningitis cohort (n = 110). Among 78 cryptococcal meningitis survivors with median CD4 count of 13 cells/μL (interquartile range: 6-44), decreased global cognitive function occurred through 12 months compared with the HIV-infected, non-cryptococcosis cohort (QNPZ-6 at 12 months, P = 0.036). Tests of performance in eight cognitive domains was impaired 1 month after cryptococcal diagnosis; however, cryptococcal meningitis survivors improved their global neurocognitive function over 12 months with residual impairment (mean z-scores < -1), only in domains of motor speed, gross motor and executive function at 12 months. There was no evidence that neurocognitive outcome was associated with initial demographics, HIV parameters, or meningitis severity. Paradoxically, persons with sterile CSF cultures after 14 days of induction amphotericin therapy had worse neurocognitive outcomes than those still culture-positive at 14 days (P = 0.002). Cryptococcal meningitis survivors have significant short-term neurocognitive impairment with marked improvement over the first 12 months. Few characteristics related to severity of cryptococcosis, including Cryptococcus burden, were associated with neurocognitive outcome.
Figures
References
-
- Ala TA, Doss RC, Sullivan CJ. Reversible dementia: a case of cryptococcal meningitis masquerading as Alzheimer's disease. J Alzheimers Dis. 2004;6(5):503–508. - PubMed
-
- Batista Leite AG, Vidal JE, Filho FB, Nogueira RS, Penalva de Oliveira AC. Cerebral infarction related to cryptococcal meningitis in an HIV-infected patient: case report and literature review. Brazilian J Infect Dis. 2004;9(2):175–179. - PubMed
-
- Bicanic T, Brouwer AE, Meintjes G, Rebe K, Limmathurotsakul D, Chierakul W, Teparrakkul P, Loyse A, White NJ, Wood R, Jaffar S, Harrison T. Relationship of cerebrospinal fluid pressure, fungal burden and outcome in patients with cryptococcal meningitis undergoing serial lumbar punctures. AIDS. 2009a;23(6):701–706. doi:10.1097/QAD.0b013e32832605fe00002030-200903270-00008 [pii. - PubMed
-
- Bicanic T, Meintjes G, Wood R, Hayes M, Rebe K, Bekker LG, Harrison T. Fungal burden, early fungicidal activity, and outcome in cryptococcal meningitis in antiretroviral-naive or antiretroviral-experienced patients treated with amphotericin B or fluconazole. Clin Infect Dis. 2007;45(1):76–80. doi:10.1086/518607. - PubMed
-
- Bicanic T, Muzoora C, Brouwer AE, Meintjes G, Longley N, Taseera K, Rebe K, Loyse A, Jarvis J, Bekker LG, Wood R, Limmathurotsakul D, Chierakul W, Stepniewska K, White NJ, Jaffar S, Harrison TS. Independent association between rate of clearance of infection and clinical outcome of HIV associated cryptococcal meningitis: analysis of a combined cohort of 262 patients. Clin Infect Dis. 2009b;49(5):702–709. doi:doi:10.1086/604716. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
