

Magnetic resonance imaging of meningiomas: a pictorial review
- PMID: 24399610
- PMCID: PMC3948902
- DOI: 10.1007/s13244-013-0302-4
Magnetic resonance imaging of meningiomas: a pictorial review
Abstract
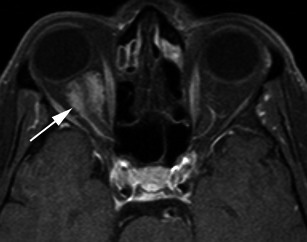
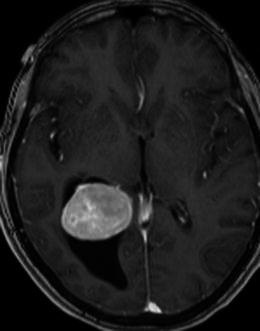
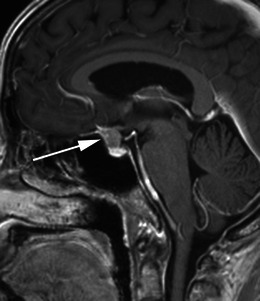
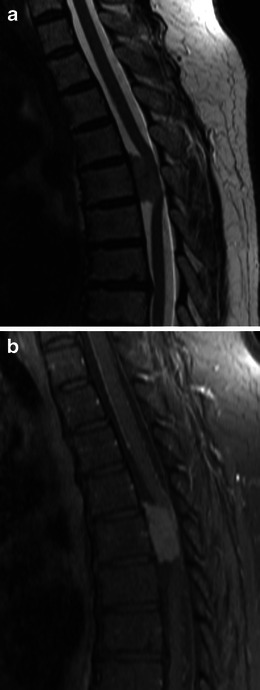
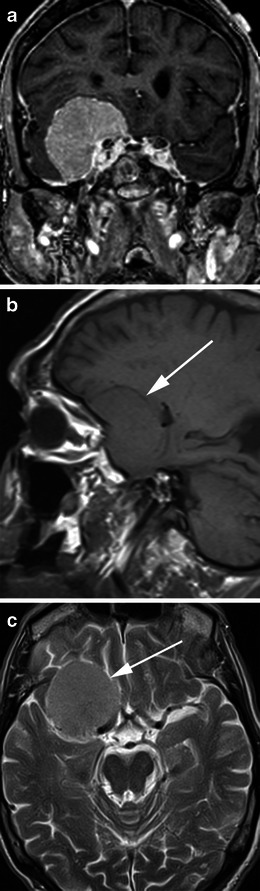
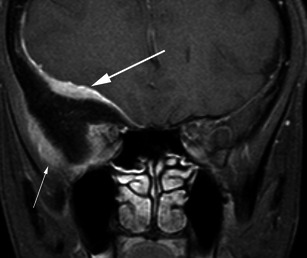
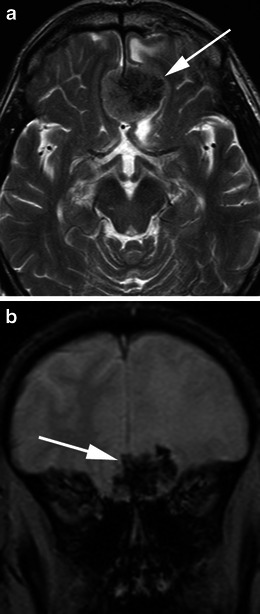
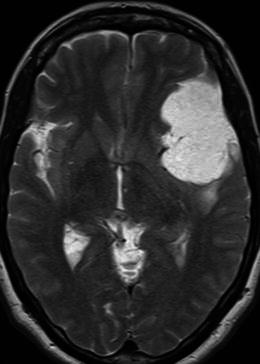
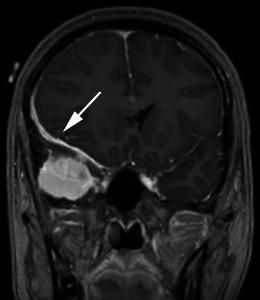
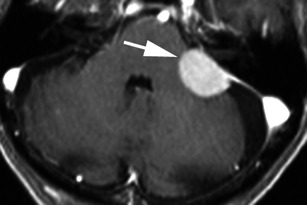
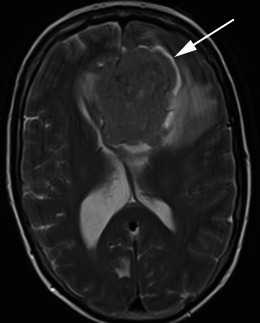
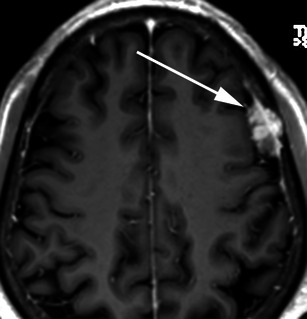
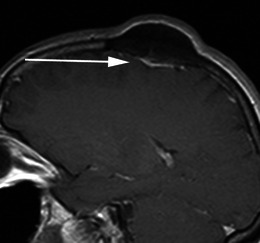
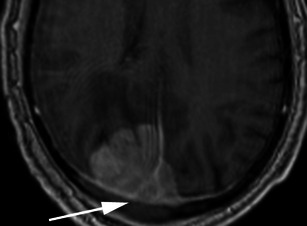
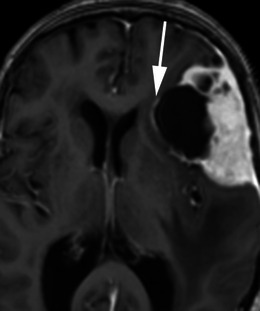
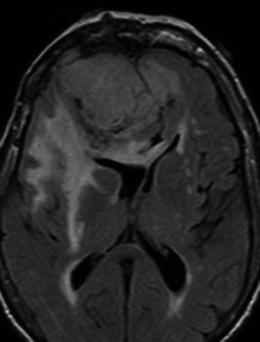
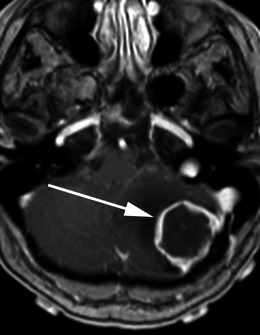
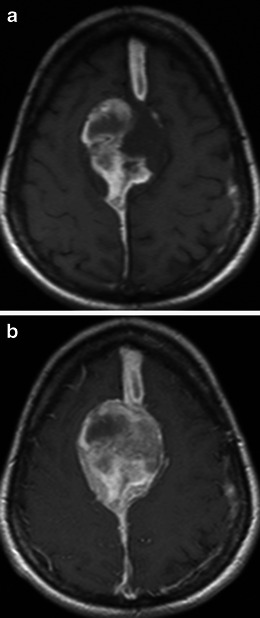
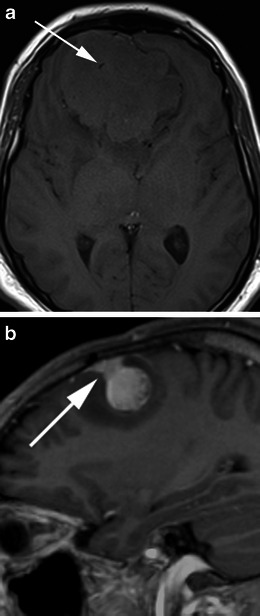
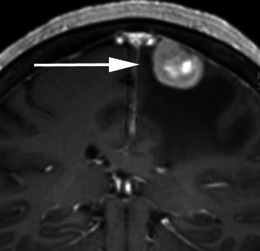
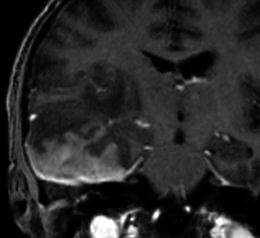
Meningiomas are the most common non-glial tumour of the central nervous system (CNS). There are a number of characteristic imaging features of meningiomas on magnetic resonance imaging (MRI) that allow an accurate diagnosis, however there are a number of atypical features that may be diagnostically challenging. Furthermore, a number of other neoplastic and non-neoplastic conditions may mimic meningiomas. This pictorial review discusses the typical and atypical MRI features of meningiomas and their mimics.
Teaching points: There are several characteristic features of meningiomas on MRI that allow an accurate diagnosis Some meningiomas may display atypical imaging characteristics that may be diagnostically challenging Routine MRI sequences do not reliably distinguish between benign and malignant meningiomas Spectroscopy and diffusion tensor imaging may be useful in the diagnosis of malignant meningiomas A number of conditions may mimic meningiomas; however, they may have additional differentiating features.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
