

Pathophysiology, management, and outcome of persistent pulmonary hypertension of the newborn: a clinical review
- PMID: 24400269
- PMCID: PMC3864198
- DOI: 10.3389/fped.2013.00023
Pathophysiology, management, and outcome of persistent pulmonary hypertension of the newborn: a clinical review
Abstract
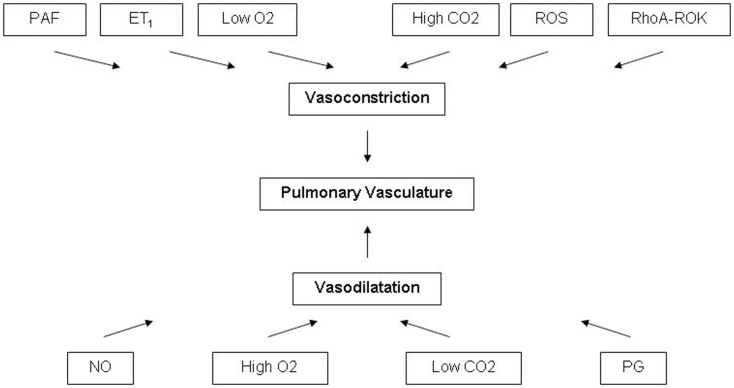
Persistent Pulmonary Hypertension of the Newborn (PPHN) results from the failure of relaxation of the pulmonary vasculature at birth, leading to shunting of non-oxygenated blood from the pulmonary to the systemic circulation. More often, full term and near-term infants are affected, however it is not uncommon to see PPHN in preterm infants who have respiratory distress syndrome. In some infants pulmonary vascular remodeling is present at birth, pointing toward the prenatal onset of the disease process. Regardless of the etiology, PPHN should be diagnosed and treated as soon as possible to avoid hypoxia related short term and long-term morbidities. The mainstay therapy is the treatment of the underlying condition along with several promising therapeutic modalities such as oxygen supplementation, mechanical ventilation, nitric oxide, phosphodiesterase inhibitors, prostaglandins analogs, endothelin receptor antagonists, and extracorporeal membrane oxygenation. The optimal approach to the management of PPHN remains controversial. After discharge from the NICU, infants with PPHN warrant long-term follow up since they are at risk for neurodevelopmental disabilities and chronic health conditions.
Keywords: newborn; outcome; pathophysiology; persistent pulmonary hypertension; treatment.
Figures
References
-
- Guyatt G, Gutterman D, Baumann M, Addrizzo-Harris D, Hylek E, Phillips B, et al. Grading strength of recommendations and quality of evidence in clinical guidelines. Chest (2006) 129:174–181 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical