

Adequacy of inhale/exhale breathhold CT based ITV margins and image-guided registration for free-breathing pancreas and liver SBRT
- PMID: 24401365
- PMCID: PMC3896695
- DOI: 10.1186/1748-717X-9-11
Adequacy of inhale/exhale breathhold CT based ITV margins and image-guided registration for free-breathing pancreas and liver SBRT
Abstract
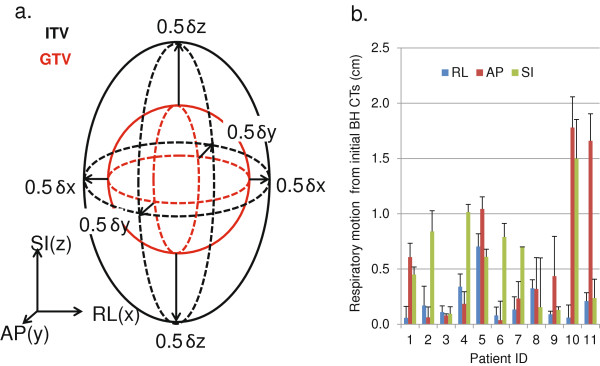
Purpose: To evaluate use of breath-hold CTs and implanted fiducials for definition of the internal target volume (ITV) margin for upper abdominal stereotactic body radiation therapy (SBRT). To study the statistics of inter- and intra-fractional motion information.
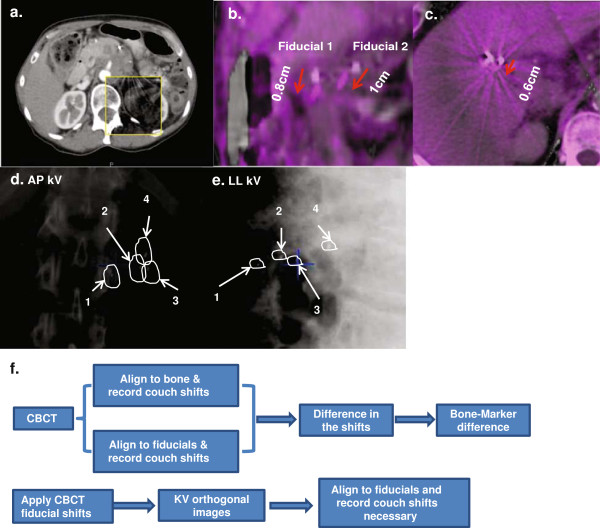
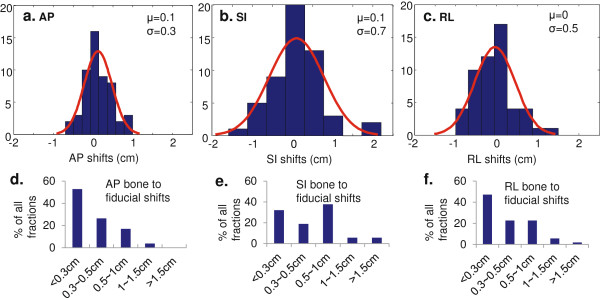
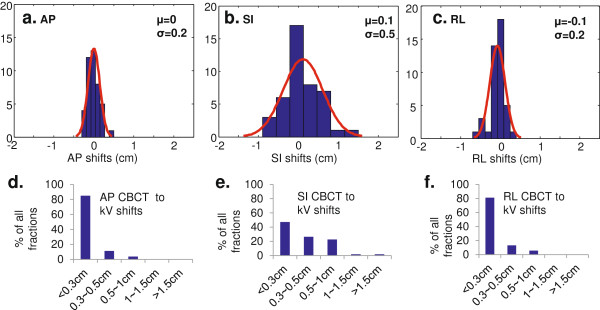
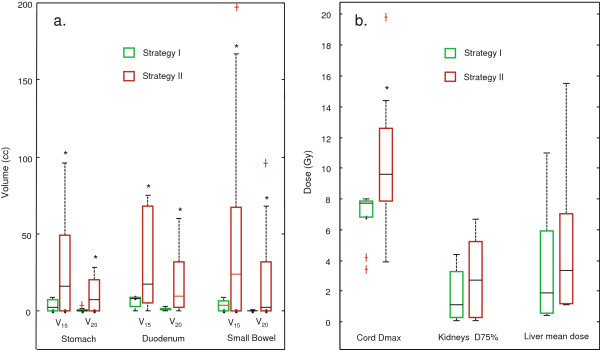
Methods and materials: 11 patients treated with SBRT for locally advanced pancreatic cancer (LAPC) or liver cancer were included in the study. Patients underwent fiducial implantation, free-breathing CT and breath-hold CTs at end inhalation/exhalation. All patients were planned and treated with SBRT using volumetric modulated arc therapy (VMAT). Two margin strategies were studied: Strategy I uses PTV = ITV + 3 mm; Strategy II uses PTV = GTV + 1.5 cm. Both CBCT and kV orthogonal images were taken and analyzed for setup before patient treatments. Tumor motion statistics based on skeletal registration and on fiducial registration were analyzed by fitting to Gaussian functions.
Results: All 11 patients met SBRT planning dose constraints using strategy I. Average ITV margins for the 11 patients were 2 mm RL, 6 mm AP, and 6 mm SI. Skeletal registration resulted in high probability (RL = 69%, AP = 4.6%, SI = 39%) that part of the tumor will be outside the ITV. With the 3 mm ITV expansion (Strategy 1), the probability reduced to RL 32%, AP 0.3%, SI 20% for skeletal registration; and RL 1.2%, AP 0%, SI 7% for fiducial registration. All 7 pancreatic patients and 2 liver patients failed to meet SBRT dose constraints using strategy II. The liver dose was increased by 36% for the other 2 liver patients that met the SBRT dose constraints with strategy II.
Conclusions: Image guidance matching to skeletal anatomy is inadequate for SBRT positioning in the upper abdomen and usage of fiducials is highly recommended. Even with fiducial implantation and definition of an ITV, a minimal 3 mm planning margin around the ITV is needed to accommodate intra-fractional uncertainties.
Figures
References
-
- Scorsetti M, Bignardi M. Conformal and stereotactic radiotherapy in hepatocellular carcinoma. Ann Ital Chir. 2008;79(2):107–110. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
