

Malignancies in HIV/AIDS: from epidemiology to therapeutic challenges
- PMID: 24401642
- PMCID: PMC4501859
- DOI: 10.1097/QAD.0000000000000071
Malignancies in HIV/AIDS: from epidemiology to therapeutic challenges
Abstract
The incidence of AIDS-defining cancers (ADCs) - Kaposi sarcoma, primary central nervous system lymphoma, non-Hodgkin lymphoma, and cervical cancer - although on the decline since shortly after the introduction of HAART, has continued to be greater even in treated HIV-infected persons than in the general population. Although the survival of newly infected people living with HIV/AIDS now rivals that of the general population, morbidity and mortality associated with non-AIDS-defining cancers (NADCs) such as lung, liver, anal, and melanoma are significant and also continue to rise. Increasing age (i.e. longevity) is the greatest risk factor for NADCs, but longevity alone is not sufficient to fully explain these trends in cancer epidemiology. In this review, we briefly review the epidemiology and etiology of cancers seen in HIV/AIDS, and in this context, discuss preclinical research and broad treatment considerations. Investigation of these considerations provides insight into why malignancies continue to be a major problem in the current era of HIV/AIDS care.
Figures
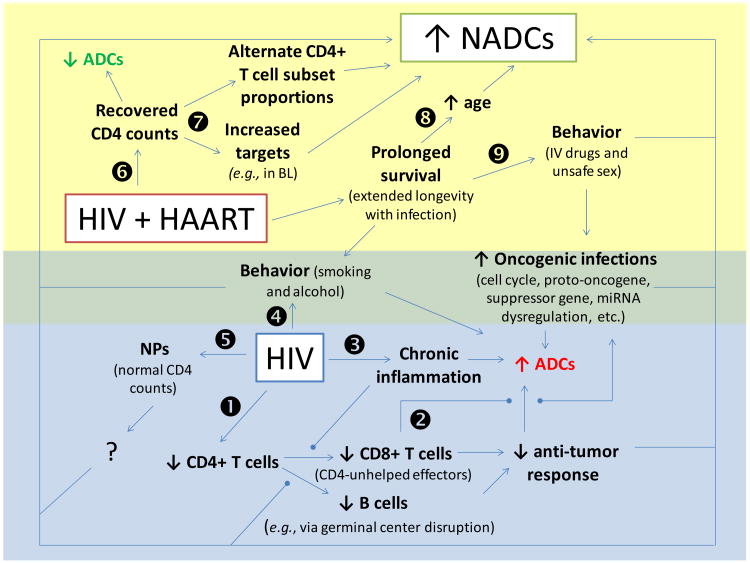
HIV infection results in the depletion of CD4 cells leading to ineffective CD4-unhelped CD8+ T effector and B cells, which results in decreased anti-tumor responses and a resultant increase in ADCs.
Lack of CD4 help leads to a lack of responses against oncogenic infections, leading to cellular and molecular dysregulation and a resultant increase in ADCs and NADCs.
HIV infection results in a state of chronic inflammation leading to a subsequent increase in ADCs and NADCs through mechanisms that are not sufficiently understood.
Behaviors increased in HIV/AIDS (e.g., smoking and alcohol overconsumption) lead to an increase in ADCs and NADCs.
Despite normal CD4 counts in non-progressors (NPs; i.e., HIV patients not requiring treatment while maintaining low/undetectable HIV viral loads for extended periods of time), NADCs continue to be increased above the level found in the non-HIV infected population.
CD4 counts recover in HIV patients treated with HAART, and a resultant decrease in ADCs is observed, but ADCs remain increased above the level found in the non-HIV infected population.
Despite recovery of total CD4 counts, the CD4+ T cell subset distribution (Th1, Th2, Th9, Th17, Th35, Treg cells, etc.) may not return to normal proportions, and increased numbers of CD4+ T cells allow for outgrowth of CD4-involved/dependent cancers.
Increased survival with HAART results in extended longevity in the context of infection leading to increased age (i.e., time for NADC outgrowth).
Increased survival with HAART results in extended time involving behaviors associated HIV/AIDS (e.g., smoking, alcohol overconsumption, IV drug use, and unsafe sex leading to oncogenic infections) and resulting in a subsequent increase in ADCs and NADCs.
References
-
- Eltom MA, Jemal A, Mbulaiteye SM, Devesa SS, Biggar RJ. Trends in Kaposi's sarcoma and non-Hodgkin's lymphoma incidence in the United States from 1973 through 1998. Journal of the National Cancer Institute. 2002;94:1204–1210. - PubMed
-
- Schneider E, Whitmore S, Glynn KM, Dominguez K, Mitsch A, McKenna MT. Revised surveillance case definitions for HIV infection among adults, adolescents, and children aged <18 months and for HIV infection and AIDS among children aged 18 months to <13 years--United States, 2008. MMWR Recommendations and reports : Morbidity and mortality weekly report Recommendations and reports / Centers for Disease Control. 2008;57:1–12. - PubMed
-
- Palella FJ, Jr, Delaney KM, Moorman AC, Loveless MO, Fuhrer J, Satten GA, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. The New England journal of medicine. 1998;338:853–860. - PubMed
-
- World Health Organization. Global summary of the AIDS epidemic. 2011 http://www.who.int/hiv/data/2012_epi_core_en.png.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
