

Self-reported head injury and risk of late-life impairment and AD pathology in an AD center cohort
- PMID: 24401791
- PMCID: PMC4057973
- DOI: 10.1159/000355478
Self-reported head injury and risk of late-life impairment and AD pathology in an AD center cohort
Abstract
Aims: To evaluate the relationship between self-reported head injury and cognitive impairment, dementia, mortality, and Alzheimer's disease (AD)-type pathological changes.
Methods: Clinical and neuropathological data from participants enrolled in a longitudinal study of aging and cognition (n = 649) were analyzed to assess the chronic effects of self-reported head injury.
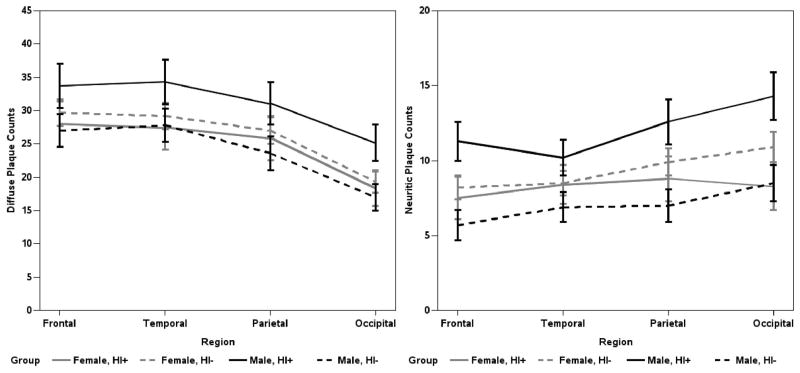
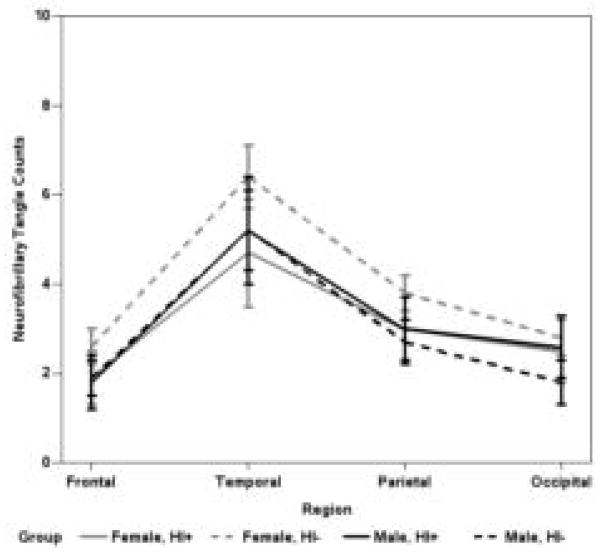
Results: The effect of self-reported head injury on the clinical state depended on the age at assessment: for a 1-year increase in age, the OR for the transition to clinical mild cognitive impairment (MCI) at the next visit for participants with a history of head injury was 1.21 and 1.34 for the transition from MCI to dementia. Without respect to age, head injury increased the odds of mortality (OR = 1.54). Moreover, it increased the odds of a pathological diagnosis of AD for men (OR = 1.47) but not women (OR = 1.18). Men with a head injury had higher mean amyloid plaque counts in the neocortex and entorhinal cortex than men without.
Conclusions: Self-reported head injury is associated with earlier onset, increased risk of cognitive impairment and dementia, increased risk of mortality, and AD-type pathological changes.
© 2013 S. Karger AG, Basel.
Figures
References
-
- McKenzie JE, Gentleman SM, Roberts GW, Graham DI, Royston MC. Increased number of βAPP-immunoreactive neurones in the entorhinal cortex after head injury. NeuroReport. 1994;6:161–4. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
