

Wound dehiscence after abdominoperineal resection for low rectal cancer is associated with decreased survival
- PMID: 24401874
- PMCID: PMC3904669
- DOI: 10.1097/DCR.0000000000000027
Wound dehiscence after abdominoperineal resection for low rectal cancer is associated with decreased survival
Abstract
Background: Abdominoperineal resection for low rectal adenocarcinoma is a common procedure with high morbidity, including perineal wound complications.
Objective: The purpose of this study was to determine risk factors for perineal wound dehiscence and to investigate the effect of wound dehiscence on survival.
Design: This was a retrospective medical chart review.
Settings: The study was conducted in a tertiary care university medical center.
Patients: Patients included in the study were those with low rectal adenocarcinoma who underwent abdominoperineal resection between January 2001 and June 2012.
Main outcomes measures: We assessed the incidence of perineal wound dehiscence, as well as survival, after surgery.
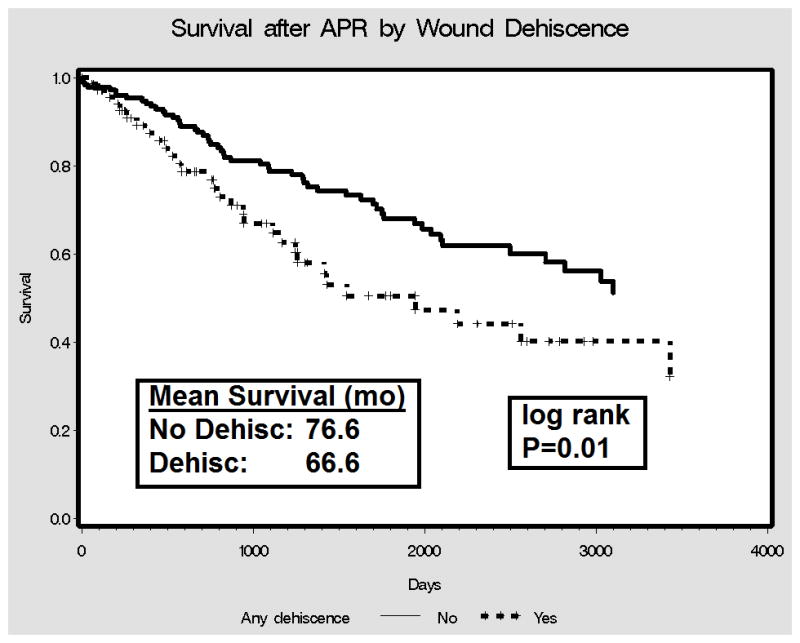
Results: A total of 249 patients underwent abdominoperineal resection for rectal carcinoma. The mean age was 62.6 years (range, 23.0-98.0 years), 159 (63.8%) were male, and the mean BMI was 27.9 (range, 16.7-58.5). There were 153 patients (61.1%) who survived for 5 years after surgery. Sixty-nine patients (27.7%) developed wound dehiscence. Multivariable analysis revealed the following associations with dehiscence: BMI (OR, 1.09; 95% CI, 1.03-1.15; p = 0.002), IBD (OR, 6.6; 95% CI, 1.4-32.5; p = 0.02), history of other malignant neoplasm (OR, 3.1; 95% CI, 1.5-6.6), and abdominoperineal resection for cancer recurrence (OR, 2.8; 95% CI, 1.2-6.3; p = 0.01). In the survival analysis, wound dehiscence was associated with decreased survival (mean survival time for dehiscence vs no dehiscence, 66.6 months vs 76.6 months; p = 0.01). This relationship persisted in the multivariable analysis (HR, 1.7; 95% CI, 1.1-2.8; p = 0.02).
Limitations: This was a retrospective, observational study from a single center.
Conclusions: The adjusted risk of death was 1.7 times higher in patients who experienced dehiscence than in those who did not. Attention to perineal wound closure with consideration of flap creation should at least be given to patients with a history of malignant neoplasm, those with IBD, those with rectal cancer recurrence, and women undergoing posterior vaginectomy. Preoperative weight loss should also reduce dehiscence risk.
Conflict of interest statement
Conflicts of Interest: None
Figures
References
-
- Garcia-Aguilar J, Hernandez de Anda E, Sirivongs P, Lee SH, Madoff RD, Rothenberger DA. A pathologic complete response to preoperative chemoradiation is associated with lower local recurrence and improved survival in rectal cancer patients treated by mesorectal excision. Dis Colon Rectum. 2003;46:298–304. - PubMed
-
- Chen ET, Mohiuddin M, Brodovsky H, Fishbein G, Marks G. Downstaging of advanced rectal cancer following combined preoperative chemotherapy and high dose radiation. Int J Radiat Oncol Biol Phys. 1994;30:169–175. - PubMed
-
- Minsky BD, Cohen AM, Enker WE, Paty P. Sphincter preservation with preoperative radiation therapy and coloanal anastomosis. Int J Radiat Oncol Biol Phys. 1995;31:553–559. - PubMed
-
- Theodoropoulos G, Wise WE, Padmanabhan A, et al. T-level downstaging and complete pathologic response after preoperative chemoradiation for advanced rectal cancer result in decreased recurrence and improved disease-free survival. Dis Colon Rectum. 2002;45:895–903. - PubMed
-
- Moore HG, Gittleman AE, Minsky BD, et al. Rate of pathologic complete response with increased interval between preoperative combined modality therapy and rectal cancer resection. Dis Colon Rectum. 2004;47:279–286. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
