

Accuracy of reports of lifetime mental and physical disorders: results from the Baltimore Epidemiological Catchment Area study
- PMID: 24402003
- PMCID: PMC4135054
- DOI: 10.1001/jamapsychiatry.2013.3579
Accuracy of reports of lifetime mental and physical disorders: results from the Baltimore Epidemiological Catchment Area study
Erratum in
-
Incorrect Wave 4 Reporting.JAMA Psychiatry. 2018 Mar 1;75(3):303. doi: 10.1001/jamapsychiatry.2017.4412. JAMA Psychiatry. 2018. PMID: 29365016 Free PMC article. No abstract available.
-
Incorrect Wave 4 Reporting.JAMA Psychiatry. 2018 Mar 1;75(3):303. doi: 10.1001/jamapsychiatry.2017.4368. JAMA Psychiatry. 2018. PMID: 29365028 No abstract available.
Abstract
Importance: Our understanding of how mental and physical disorders are associated and contribute to health outcomes in populations depends on accurate ascertainment of the history of these disorders. Recent studies have identified substantial discrepancies in the prevalence of mental disorders among adolescents and young adults depending on whether the estimates are based on retrospective reports or multiple assessments over time. It is unknown whether such discrepancies are also seen in midlife to late life. Furthermore, no previous studies have compared lifetime prevalence estimates of common physical disorders such as diabetes mellitus and hypertension ascertained by prospective cumulative estimates vs retrospective estimates.
Objective: To examine the lifetime prevalence estimates of mental and physical disorders during midlife to late life using both retrospective and cumulative evaluations.
Design, setting, and participants: Prospective population-based survey (Baltimore Epidemiologic Catchment Area Survey) with 4 waves of interviews of 1071 community residents in Baltimore, Maryland, between 1981 and 2005.
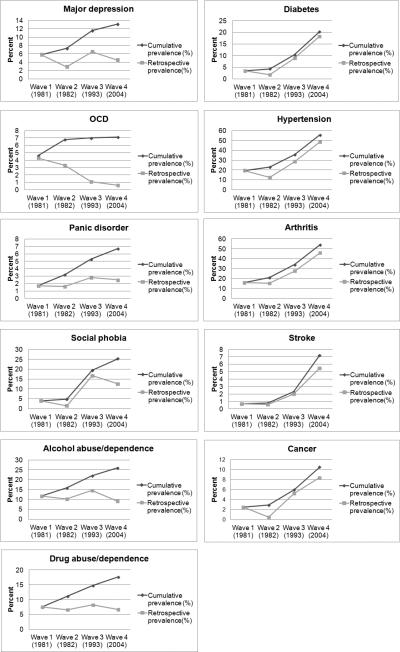
Main outcomes and measures: Lifetime prevalence of selected mental and physical disorders at wave 4 (2004-2005), according to both retrospective data and cumulative evaluations based on 4 interviews from wave 1 to wave 4. RESULTS Retrospective evaluations substantially underestimated the lifetime prevalence of mental disorders as compared with cumulative evaluations. The respective lifetime prevalence estimates ascertained by retrospective and cumulative evaluations were 4.5% vs. 13.1% for major depressive disorder, 0.6% vs. 7.1% for obsessive-compulsive disorder, 2.5% vs. 6.7% for panic disorder, 12.6% vs. 25.3% for social phobia, 9.1% vs. 25.9% for alcohol abuse or dependence, and 6.7% vs. 17.6% for drug abuse or dependence. In contrast, retrospective lifetime prevalence estimates of physical disorders ascertained at wave 4 were much closer to those based on cumulative data from all 4 waves. The respective prevalence estimates ascertained by the 2 methods were 18.2% vs. 20.2% for diabetes, 48.4% vs. 55.4% for hypertension, 45.8% vs. 54.0% for arthritis, 5.5% vs. 7.2% for stroke, and 8.4% vs. 10.5% for cancer.
Conclusions and relevance: One-time, cross-sectional population surveys may consistently underestimate the lifetime prevalence of mental disorders. The population burden of mental disorders may therefore be substantially higher than previously appreciated.
Figures
Comment in
-
Accuracy in reporting past psychiatric symptoms: the role of cross-sectional studies in psychiatric research.JAMA Psychiatry. 2014 Mar;71(3):233-4. doi: 10.1001/jamapsychiatry.2013.4111. JAMA Psychiatry. 2014. PMID: 24401961 No abstract available.
References
-
- Kessler RC, McGonagle KA, Zhao S, et al. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the united states. results from the national comorbidity survey. Arch Gen Psychiatry. 1994;51(1):8–19. - PubMed
-
- Andrade L, Walters EE, Gentil V, Laurenti R. Prevalence of ICD-10 mental disorders in a catchment area in the city of sao paulo, brazil. Soc Psychiatry Psychiatr Epidemiol. 2002;37(7):316–325. - PubMed
-
- Fergusson DM, Horwood LJ. The christchurch health and development study: Review of findings on child and adolescent mental health. Aust N Z J Psychiatry. 2001;35(3):287–296. - PubMed
-
- Vollebergh WA, Iedema J, Bijl RV, de Graaf R, Smit F, Ormel J. The structure and stability of common mental disorders: The NEMESIS study. Arch Gen Psychiatry. 2001;58(6):597–603. - PubMed
-
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry. 2005;62(6):593–602. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
